ADOLESCENT HEALTH LITERACY AND
SOCIAL INEQUALITY IN HEALTH:
RESULTS FROM THE FLEMISH HEALTH
BEHAVIOUR
IN
SCHOOL-AGED
CHILDREN (HBSC) STUDY
Word count: 7.035Maxim Van den broecke
Student number: 01309548
Supervisor: Dr. Katrijn Delaruelle
Cosupervisor: Mr. Maxim Dierckens
A dissertation submitted to Ghent University in partial fulfilment of the requirements for the degree of Master of Science in Health Promotion
ADOLESCENT HEALTH LITERACY AND
SOCIAL INEQUALITY IN HEALTH:
RESULTS FROM THE FLEMISH HEALTH
BEHAVIOUR
IN
SCHOOL-AGED
CHILDREN (HBSC) STUDY
Word count: 7.035Maxim Van den broecke
Student number: 01309548
Supervisor: Dr. Katrijn Delaruelle
Cosupervisor: Mr. Maxim Dierckens
A dissertation submitted to Ghent University in partial fulfilment of the requirements for the degree of Master of Science in Health Promotion
Table of contents
Acknowledgements ... 3
Introduction ... 4
Abstract ... 7
Literature review ... 9
1. The concept of health literacy ... 9
2. The relationship between health literacy and health ... 10
3. The relationship between socioeconomic status and health and the role of health literacy ... 11
4. Adolescent health literacy ... 13
5. Research questions ... 15 Method ... 16 1. Sample ... 16 2. Measures ... 17 2.1 Dependent variables ... 17 2.2 Independent variables ... 18 3. Statistical analysis ... 19 Results ... 20 1. Multilevel models ... 21
1.1 STRS and MVPA regressed on HL. ... 21
1.2 STRS and MVPA regressed on parental education. ... 21
1.3 STRS and MVPA regressed on parental education and HL. ... 22
Discussion ... 24
1. Adolescent health literacy and health behaviors ... 24
2. SES and adolescent health behaviors ... 25
3. Adolescent health literacy and socioeconomic differences in health behaviors ... 26
4. Strengths and limitations ... 26
Conclusions ... 28
Relevance for practice and recommendations ... 28
References ... 30
Acknowledgements
First of all, I would like to express my gratitude to my supervisor and cosupervisor, Dr. Katrijn Delaruelle and Mr. Maxim Dierckens. Without their intense guidance and encouragement this thesis would never have been accomplished. During the process of writing this dissertation I have encountered several difficulties. The extensive feedback and willingness to help, provided by Dr. Delaruelle and Mr. Dierckens, have been essential in overcoming the obstacles I encountered while constructing this thesis.
Furthermore, I would like to thank my family for giving me the energy to persevere and complete this work. I specifically want to thank my father, whose ongoing support during this endeavor has been indispensable.
Lastly, I want to thank my close friends as their companionship has helped me to keep a level head during this process.
Introduction
The existence of social inequalities in health has long been acknowledged (Mackenbach, 2006). Such inequalities refer to systematic differences in health witnessed between groups differentiated by socioeconomic measures. Among others, earlier studies have documented that individuals from lower socioeconomic background have higher mortality and morbidity rates as compared to individuals from lower socioeconomic backgrounds (Feinstein, 1993; Adler & Newman, 2002) In addressing these social health inequalities, early intervention and prevention are crucial (Manganello, 2008). Promoting healthy lifestyle behaviors (e.g. physical activity, healthy diet) and preventing harmful lifestyle behaviors (e.g. smoking, sedentary behavior) in adolescents marks an important strategy to tackle health inequalities across the lifespan (Brodersen, Steptoe, Boniface, & Wardle, 2007; Marmot & Bell, 2012), as these behaviors have been associated with the presence of non-communicable diseases (NCDs) in later life (EU, 2017). NCDs are estimated to be responsible for almost 87% of DALYs (disability-adjusted life years) and 91% of deaths in the EU. Approximately 46% of DALYs and 61% of deaths can be attributed to risk factors such as unhealthy diet, tobacco use, harmful use of alcohol and physical inactivity (Stanaway et al., 2018). Both the distribution and the impact of NCDs and their risk factors are highly inequitable. Adolescents with lower socioeconomic backgrounds more often exhibit these risk factors compared to adolescents with higher socioeconomic backgrounds (Lowry et al., 1996; Hanson & Chen, 2007). As adolescent health behaviors are often translated into adulthood, adolescents are considered as valuable targets for interventions aimed at reducing social health inequalities across the lifespan (Europe et al., 2019). The present study therefore focuses on health behaviors in an adolescent population. In the past decades, health care practitioners, researchers and policymakers have recognized health literacy (HL) as a potentially important pathway to reduce social inequalities in health behaviors (Saha, 2006; WHO, 2013; Stormacq, Van den Broucke, & Wosinski, 2019). The notion that HL may be an important pathway originated from the acknowledgement of interrelationships among socioeconomic status (SES), HL and health behaviors (Saha, 2006; Stormacq et al., 2019). Persons with lower SES on average report lower HL compared to persons with higher SES (Paasche-Orlow & Wolf, 2007). In addition, HL and SES have been linked to several health behaviors (Hanson & Chen, 2007; Berkman et al., 2011). However, these studies mainly focus on an adult population, whereas adolescent HL is often disregarded (Fleary et al., 2018). Studies associating adolescent health behaviors with either SES, HL or both have not yet produced
consistent evidence. Additionally, only a few studies have attempted to construct HL concepts and instruments specifically for adolescents (L. Paakkari & Paakkari, 2012; Paakkari, Torppa, Kannas, & Paakkari, 2016; Connelly & Turner, 2017). Furthermore, to the best of our knowledge, no studies to date have examined whether HL is a driving mechanism behind social inequalities in adolescents’ health behaviors. The current study aims to address this shortcoming by examining whether HL explains part of the association between SES and health behaviors in adolescents (i.e. main research question). As the evidence regarding the relationships between both SES as well as HL and adolescent health behaviors lacks consistency, the present study will additionally examine these associations.
The data for the present study is provided by the Flemish 2017/2018 Health Behaviour in School-aged Children (HBSC) study. Within the HBSC study, data was collected on adolescents and their health behaviors. Data from the study shows that the vast majority of Flemish adolescents do not meet the recommended guidelines for both physical activity and sedentary behavior. Flemish adolescents on average display too much sedentary behavior and too little physical activity (Dierckens, De Clerq, & Deforche, 2019). These adolescent health behaviors have been linked to a variety of negative health outcomes throughout the lifespan (Haskell et al., 2009; Tremblay et al., 2011) as well as to SES (Brodersen et al., 2007). Additionally, physical activity has been previously been significantly associated with HL in adolescents (Levin-Zamir et al., 2011). Within the current study, physical activity and sedentary behavior were selected to be examined. The choice of these health behaviors was motivated by the above mentioned associations and by the failure of the average Flemish adolescent to meet recommended guidelines on both physical activity and sedentary behavior.
In sum, the main research question is: “Does adolescent HL partly explain the relationship between SES and health behaviors in adolescents?”. Additionally, two other research questions are posed: “Is HL significantly associated with health behaviors in adolescents?” and “Is there significant relationship between SES and health behaviors in adolescents?”.
First, HL as a potential mediator of socioeconomic inequalities in adolescent health behaviors is discussed in the literature review. The concept of HL is explored and its health-related outcomes are presented. This is followed by a description of SES, its health-related outcomes and the role of HL in these relationships. Next, adolescent HL and its relevance as a distinct concept is explained. Throughout the literature review, a specific focus is placed on adolescence and health behaviors.
Based on the information presented, the literature review concludes by formulating several relevant research questions as well as specific hypotheses. Thereafter, the used data and its collection is described in the methodology section. In this part of the thesis, the used variables and data analyses are explained as well. Next, classified according to the research questions, the results from the analyses are described in detail. Interpretation of these results and their links to relevant literature are explicated in the discussion section. Finally, the most important results, their relevance for future practice and recommendations for further research are summarized in the conclusion.
Fieldwork was conducted by the author of this thesis at the University of Ghent. This consisted in helping to prepare factsheets for the 2017/2018 HBSC study (Appendix E).
Abstract
Background & objective: Addressing social inequalities in adolescent health behaviors is often
described as a means to reduce health inequalities across the lifespan.
However, in order to address these social inequalities in adolescent health behaviors, researchers should gain understanding of the mechanisms behind this association. The current study focuses on health literacy (HL) as a mediator of socioeconomic status (SES) differences in adolescent health behaviors. HL has been identified as a mediator among adults, but studies among adolescents are absent. The main purpose of this thesis therefore was to examine whether HL partly explains SES (parental education) differences in health behaviors (physical activity and sedentary behavior) in adolescents. Additionaly, the associations between adolescent health behaviors and both SES and HL were examined.
Methods: Multiple regression analyses were performed on data from adolescents (N = 9358)
provided by the 2017/2018 Flemish HBSC study. A multilevel approach was used to account for clustering at the school level.
Results: Adolescent HL and SES were signifcantly associated with health behaviors. Adolescents
with low HL and low SES reported less physical activity and more sedentary behavior. Moreover, the study showed that HL partly explains the relationship between SES and health behaviors in adolescents.
Conclusion: These findings suggest that interventions aimed at tackling socioeconomic health
inequalities among adults can benefit from a strong focus on adolescent HL. The present study forms a basis for further research focusing on adolescent HL, the relationship between adolescent health behaviors and both SES and HL, and HL’s role in SES differences in adolescent health behaviors.
Amount of words article: 7.035 (exclusive acknowledgements, table of content, introduction, abstract, figures, tables, reference table and appendices)
Abstract
Achtergrond & doelstelling: Het aanpakken van sociale ongelijkheden in gezondheidsgedragingen
bij adolescenten wordt vaak omschreven als een manier om gezondheidsongelijkheden over alle leeftijden heen te verkleinen. Om deze sociale ongelijkheden in adolescente gezondheidsgedragingen aan te pakken moeten onderzoekers een beter inzicht krijgen in de mechanismen achter deze relatie. De huidige studie focust zich op gezondheidsgeletterdheid als zijnde een mediator in de relatie tussen socio-economische status (SES) en adolescente gezondheidsgedragingen. In tegenstelling tot bij adolescenten, werd bij volwassenen gezondheidsgeletterdheid reeds geïdentificeerd als mediator. Het hoofddoel van deze thesis was daarom om te onderzoeken of gezondheidsgeletterdheid een deel van de relatie tussen SES (opleidingsniveau ouders) en gezondheidsgedragingen (fysieke activiteit en sedentair gedrag) bij adolescenten verklaart. Tevens werden verbanden tussen adolescente gezondheidsgedragingen en zowel SES als gezondheidsgeletterdheid onderzocht.
Methode: Meervoudige regressieanalyses werden uitgevoerd op data van adolescenten verkregen
uit de 2017/2018 Vlaamse HBSC studie. Een multilevel benadering werd gebruikt om rekening te houden met het voorkomen van clusters op school-niveau.
Resultaten: Zowel SES als gezondheidsgeletterdheid hadden een significant effect op adolescente
gezondheidsgedragingen. Adolescenten met een lage gezondheidsgeletterdheid en lage SES rapporteerden minder fysieke activiteit en meer sedentair gedrag. Bovendien werd aangetoond dat gezondheidsgeletterdheid een deel van de relatie tussen SES en gezondheidsgedragingen verklaart.
Conclusie: Deze bevindingen wijzen aan dat bij interventies gericht op het verkleinen van
socio-economische gezondheidsongelijkheden in volwassenen, een sterke focus op
gezondheidsgeletterdheid bij adolescenten voordelig kan zijn. De huidige studie legt de basis voor vervolgonderzoek dat kan focussen op gezondheidsgeletterdheid bij adolescenten, de relatie tussen adolescente gezondheidsgedragingen en zowel SES als gezondheidsgeletterdheid, en de rol van gezondheidsgeletterdheid bij SES verschillen in adolescente gezondheidsgedragingen.
Literature review
1. The concept of health literacy
To understand health literacy (HL) as a distinct concept, in-depth knowledge of literacy itself is required. In defining literacy, the National Assessment of Adult Literacy (NAAL), a national representative assessment of English literacy among American adults aged 16 and older, is often cited (Nutbeam, 2009). Within the scope of the NAAL, literacy is comprised of both task-based and skill-based literacy (National Assessment of Adult Literacy, 2003). Task-based literacy encompasses key literacy tasks such as being able to read and write a basic text. Skill-based literacy involves the knowledge and skills required to execute these tasks. However, in situations where specific content knowledge (e.g. health knowledge) is required, a higher level of literacy (both task- and skill-based) does not render a person able to understand information in written text. Similarly, in situations where the context (e.g. health care environment) is unfamiliar the same logic applies (Nutbeam, 2009). This growing awareness supported the development of new “literacies” as distinct concepts where content- and context-specific knowledge are requisites (Coiro, 2003). The concept of HL, which requires content-specific literacy in a health context, can be seen as emerging from this notion.
Several efforts have been made to conceptualize HL (Sørensen et al., 2012). Ratzan and Parker (2000, p. 6) defined HL as “the degree to which individuals have the capacity to obtain, process,
and understand basic health information and services needed to make appropriate health care decisions.” This widely adopted definition was further refined by Nutbeam (2000), classifying HL
into three categories: functional, communicative and critical HL. Functional HL is defined by basic writing and reading abilities needed to obtain, process and use factual health information (e.g. health risks, medication prescriptions, health care system). Communicative HL comprises more advanced skills (e.g. derive meaning from different sources of communication) needed to apply health-related information to changing contexts. Nutbeam’s third category, critical HL, is described as the ability to be effective in analyzing information and applying that information to exert greater control over life events situations.
In the past two decades, research examining HL has grown exponentially. Many disciplines have focused on the concept of HL, including health educators promoting HL, health economist focusing on HL as a means to promote equality in health, public HL for lawyers (Sørensen et al., 2012). However, most of these studies have merely focused on adult HL (Okan, Bauer, Levin-Zamir, et
al., 2019) while disregarding children and adolescents as a target group (Bröder et al., 2017). Only recently, attention has been given to adolescent HL (Ormshaw et al., 2013). Few HL conceptualizations and definitions have been constructed specific to adolescents. These concepts most frequently address adolescent’s HL through focus on their parents or care taker’s HL (DeWalt & Hink, 2009; Connelly & Turner, 2017) or as skills-centered outcomes of school-education (e.g. reading and writing ability, theoretical knowledge, critical thinking) (L. Paakkari & Paakkari, 2012). The latter commonly uses performance-based instruments in a school setting for measuring HL, hereby detaching HL from real-life actions or behavior. Studies examining HL of adolescents through the assessment of their parents or care-takers’ HL do so based on the notion that they are the main source of health information and education for adolescents (Okan et al., 2018). In addition, parents contribute significantly to adolescents’ management of disease, entry into the health system and health decision-making in general (Forrest et. al, 1997, as cited in Okan et al., 2018). However, there is limited evidence supporting the assessment of adolescent HL by measuring their parents or care-taker’s HL (Okan et al., 2018). One more important shortcoming of recent adolescent HL research is that it has yet to explore development-focused perspectives, recognizing different life phase particularities characteristic to adolescence (Okan, Bauer, Levin-Zamir, et al., 2019). These shortcomings highlight the importance of developing new, more comprehensive theoretical frameworks of HL that take characteristics of specific target groups into consideration (e.g. adolescents).
To date, the majority of research into HL, its influencing factors and its relation to health outcomes has used validated instruments based on Nutbeam’s (2009) definition of functional HL (Haun et al., 2014). In what follows, Nutbeam’s (2009) definition, containing three categories (functional, communicative and critical HL), will be used when describing HL.
2. The relationship between health literacy and health
A vast amount of research has established significant associations between HL and a wide range of health-related outcomes among adults (Institute of Medicine (US) Committee on Health Literacy, 2004). Low HL scores are associated with increased use of health care services, such as hospitalizations and emergency care use, and decreased use of preventive services (e.g. mammography screening, influenza immunizations) (Berkman et al., 2011). Adults with low HL report more difficulties in appropriately using prescription medication (Kripalani et al., 2006). In addition, having low HL is related to an increased likelihood of displaying symptoms of depression and reporting poorer self-rated health (Wolf, Gazmararian, & Baker, 2005; Bennett, Chen, Soroui,
& White, 2009). Among elderly persons, low HL predicts higher all-cause mortality and
cardiovascular death rates (D. W. Baker et al.,s2007).
However, the majority of research into HL has disregarded health-related behavioral outcomes, with the exception of the use and compliance of health care services (including preventive services) (Berkman et al., 2011). Only a limited amount of research has examined the relationship between HL and healthy or harmful lifestyle behaviors (Geboers et al., 2016). For instance, in a national sample of British adults, persons with high HL reported more fruit and vegetable intake and were less likely to be smokers (von Wagner et al., 2007). Lower HL in older adults is associated with insufficient physical activity (Geboers et al., 2016).
The above-mentioned health-related outcomes apply mainly to adults and elderly persons. Similar research identifying adolescents as a specific target group remains scarce. Fleary, Joseph, & Pappagianopoulos (2018) systematically reviewed and synthesized literature on the relation between HL and health behaviors in adolescents. Eleven studies reported significant associations between HL and health behaviors in adolescents after controlling for demographics. Higher HL was related to a healthier diet, more exercise (Levin-Zamir et al., 2011) and less tobacco and alcohol use (Fleary et al., 2018). However, in the relationship between HL and physical activity, significant associations are not found consistently across all studies (Fleary et al., 2018). These inconsistencies may reflect the absence of a unanimously accepted, comprehensive theoretical framework for HL that considers particularities of specific target groups (e.g. developmental characteristics of adolescents) (Okan, Bauer, Pinheiro, et al., 2019). Despite recent efforts, adolescent HL, health behavioral outcomes of HL, and especially health behavioral outcomes of adolescent HL remain understudied to date (Fleary et al., 2018).
3. The relationship between socioeconomic status and health and the role of
health literacy
The relationship between socioeconomic status (SES) and health outcomes has been well documented: individuals from lower socioeconomic backgrounds generally report greater burden of disease, higher overall mortality, and higher susceptibility to diseases as compared to individuals from higher socioeconomic backgrounds. (Antonovsky, 1967;Syme & Berkman, 1976; Mackenbach & Kunst, 1997; Mackenbach, Kunst, Cavelaars, Groenhof, & Geurts, 1997). Additionally, many studies have revealed a social gradient in health behaviors (Petrovic et al.,
2018). For instance, In both adults and adolescents, low SES is related to increased tobacco use and sedentary behavior. Decreased physical activity (Brodersen et al., 2007) and fruit and vegetable intake are more common in adults and adolescents reporting low SES (Lowry, Kann, Collins, & Kolbe, 1996; Parks, Housemann, & Brownson, 2003; Hanson & Chen, 2007). However, in adolescents, socioeconomic differences in physical activity and sedentary behavior are not found consistently across all studies (Stalsberg & Pedersen, 2010; Mielke, Brown, Nunes, Silva, & Hallal, 2017). As these health-damaging behaviors (e.g. tobacco use, physical inactivity, sedentary behavior) have been found to be socially patterned, they contribute to social inequalities in overall health (Pampel et al., 2010). However, it should be noted that social inequalities in health involve more than health behaviors (Lantz et al., 1998; Petrovic et al., 2018). Nevertheless they still account for an important amount of social inequalities in health. Interventions aimed at health behaviors therefore mark an important strategy to increase population health and reduce social health inequalities (Pampel et al., 2010; Petrovic et al., 2018).
Several mechanisms have been documented that link SES to health behaviors. Examples include the availability of resources, harmful health behaviors as coping mechanisms for deprivation and stress linked to lower socioeconomic background, the adoption of health behaviors as a means for class distinction and knowledge and access to information about health risks (Pampel et al., 2010). In the present study, the latter is examined by focusing on HL. In the past, attention has been given to HL as a mechanism relating SES to other health-related outcomes and health in general as well (Stormacq et al., 2019).
HL and SES are both related to a wide range of health-related outcomes and SES measures are associated with HL. Individuals with lower socioeconomic backgrounds on average have lower HL compared to individuals with higher socioeconomic backgrounds (Paasche-Orlow & Wolf, 2007). Recognition of these interrelationships incited Saha (2006) to present HL as a possible important target to reduce social health inequalities. This suggestion has been recognized and translated into policy since before the start of the 21st century (Nutbeam & Kickbusch, 2000) and has since then
not been refuted. Health policies from several national and international governments and institutions have identified HL as a priory public health goal to reduce social inequalities in health (Australia. Department of Health et al., 1993; Health, 1999; EU, 2007; WHO, 2008).
Studies examining HL’s role in socioeconomic differences in health-related outcomes most frequently use educational level as measure for SES (Stormacq et al., 2019). Education influences
both occupation and income, therefore the choice of educational level as SES parameter seems justified (O’Neill et al., 2014). Only a small amount of studies have investigated this mediating role of HL in socioeconomic health inequalities. In these studies, HL was consistently presented as a significant mediator between educational level and both health outcomes as well as health-related behaviors (Stormacq et al., 2019). Worse self-rated physical, mental and general health were observed in persons with a lower educational level and lower HL. Though differing in effect size, HL was observed to partly mediate the relationship between educational level and these three health outcomes (van der Heide et al., 2013). These results confirm the findings from Bennett et al. (2009) where HL partly explained educational differences in self-reported health status. Howard, Sentell, & Gazmararian (2006) presented similar results among older adults. Research into the association between educational level and glycemic control in diabetes patients also confirmed HL’s mediating role (Schillinger et al., 2006). Examining hypertension control as a health outcome produced the same results, though HL only minimally explained the relationship with educational level (Pandit et al., 2009).
Friis, Lasgaard, Rowlands, Osborne, & Maindal (2016) were first in examining socioeconomic differences in health behaviors and the mediating role of HL. Health behaviors subjected to research were smoking, physical activity and dietary habits. Within this Danish population-based study, HL was measured with two different HL scales. Only one significantly mediated the relationship between educational level and the included health behaviors (Friis et al., 2016). Park et al. (2018) used a different HL measure to identify HL as a mediator of educational differences in physical activity, fruit and vegetable intake and sedentary behavior. Only in investigating sedentary behavior was HL not found to significantly mediate the relationship between health behavior and educational level (Park et al., 2018). It is important to note that no consistent use of one HL instrument and definition can be observed in the aforementioned studies. Research into HL’s contribution to socioeconomic, and more specifically, educational differences in health-related outcomes remains limited. Studies focusing on health behaviors as outcomes remain even more so (Stormacq et al., 2019). To the best of our knowledge, similar studies identifying adolescents as a specific target group have yet to be conducted.
4. Adolescent health literacy
Adolescence marks an important period in life. Development of independent decision-making takes place in this stage (Ghanbari et al., 2016). Adolescence is characterized by critical stages of
development based on many physical, emotional and cognitive changes (Keating, 1990, as cited in Ghanbari et al., 2016). Enabling adoscelents to have more control over their health status and providing them with accurate and reliable information supports the development of lifelong healthy behavior (Ghanbari et al., 2016). Furthermore, adolescent health behavior often translates into adult health behavior and disease risks (Fleary et al., 2018). This has been well documented in regard to several health behaviors and diseases. For example, obesogenic health behavior (e.g. physical activity, sedentary behavior, dietary behavior) in adolescents risks translating into adult obesity and obesity-related health complications. Adolescent alcohol use is associated with mental health problems, chronic diseases and alcohol-related disorders in adulthood. Increased risk for cancer, cardiovascular diseases and increased likelihood of nicotine-dependency is witnessed in individuals who take up smoking in adolescence (Fleary et al., 2018). These examples show that addressing health behaviors in adolescence marks an important strategy to combat health inequalities not only in adolescence, but across the lifespan (Europe et al., 2019). Additionaly, the vast majority of adolescents can be reached through well organised school-based programmes and interventions. This availability of an appropriate setting for intervention further strengthens the importance of adolescents as a target population for improving health-related outcomes (Europe et al., 2019).
By focusing on HL at an early age, inequalities in harmful health behaviors can be reduced. In doing so, positive health outcomes in later life can be attained (Fleary et al., 2018). Extra attention for adolescent HL is warranted due to the fact that adolescents are given a large amount of educational material by health care providers, schools and intervention programs (Manganello, 2008). Despite this, the importance of adolescent HL is often disregarded (Chisolm & Buchanan, 2007). Few studies concerning HL have focused on adolescents over the past decades (Okan et al., 2018). As a result, HL conceptualizations and instruments have seldom been constructed specifically for this target group. Though efforts have been made (L. Paakkari & Paakkari, 2012; Connelly & Turner, 2017), research into theoretical frameworks and measures for adolescent HL, as of yet, has failed to include development-focused perspectives (Fleary et al., 2018).
As mentioned before, recent studies have demonstrated that HL mediates the relationship between SES, and particularly educational level, and a variety of health-related outcomes such as health behaviors (Friis et al., 2016; Stormacq et al., 2019). These studies examined HL’s mediating role in adult populations and to the best of our knowledge, no similar studies have been conducted specific to adolescent populations thus far.
5. Research questions
Addressing adolescent health behaviors is recognized as an important approach in reducing social health inequalities across the life-span (Europe et al., 2019). The present study therefore aims to examine whether HL partly explains the relationship between SES and health behaviors in adolescents. To add to the growing body of evidence, this study will additionally examine the relationship between adolescent health behaviors and both HL as well as SES. In sum, the following research questions are examined:
- Is HL significantly associated with health behaviors in adolescents?
- Is there a significant relationship between SES and health behaviors in adolescents? - Does HL partly explain the relationship between SES and health behaviors in adolescents? In line with existing research, a significant relationship between HL and adolescent health behaviors is expected to be found. In regard to the relationship between SES and health behaviors, a significant association is hypothesized. As for the main research question, similar to research in adult populations, HL is expected to partly explain the effects SES on health behaviors in adolescents.
Method
1. Sample
Individual-level data were obtained from the 2017/2018 Flemish Health Behavior in School-aged Children (HBSC) study. Originally set up by England, Finland and Norway, the HBSC study was adopted in 1983 by the WHO Regional Office for Europe as a collaborative study. To date, the HBSC research network includes 49 countries and regions across Europe and North America. Every four years, the HBSC-study collects data on 11-, 13- and 15-year old boys’ and girls’ health behaviors, health and well-being (Inchley, Currie, Cosma, & Samdal, 2018). In addition to data on 11-, 13- and 15-year old boys and girls, the Flemish HBSC study expanded the age range to include data on adolescents in higher cycles of primary and secondary schools. This last expansion enables researchers to gain insights into students who have progressed further in adolescence. Standardized questionnaires, conform to the international HBSC study protocol (Inchley et al., 2018), were filled out by students within a class-setting under supervision of a teacher or another staff member. In collecting the data in the HBSC-study, cluster probability sampling was used. Therefore, results from students within the same school may not be seen as independent of each other as responses may be more alike than those of students in general. To take into account the effects of cluster sampling a minimal sample size of 1500 students per age group was determined (Inchley et al., 2018). In Flanders, the data-collection for the 2017/2018 HBSC study took place between February 2018 and June 2018. Participation was voluntary and anonymous. Parents were notified in advance by letter and refusal to participate was possible. The study was approved by the ethics committee of the Ghent University Hospital amendment (EC UZG/2013/1145).
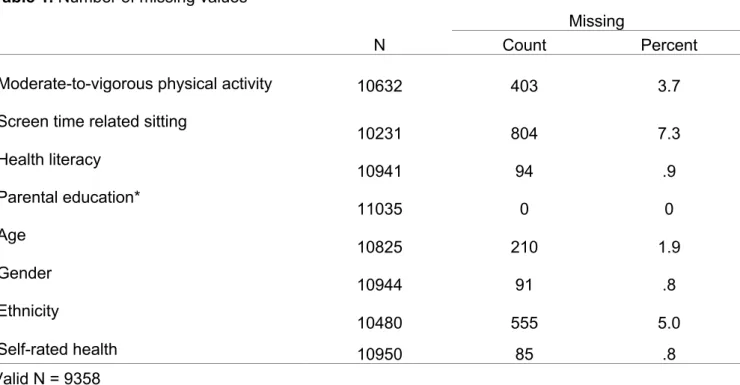
In total, 194 schools participated, representing a response rate at the school-level of 21.6%. At the individual-level (i.e. students), the data-set includes 11 035 students, representing a response rate of 72.2%. In the present analyses, students with missing values for at least one of the individual-level measures described below, were excluded (total missing cases = 1677). The proportion of missing values for each variable ranged from 0.8% to 7.3%. The number of missing values for each included variable can be found in appendix A. The final dataset contained 9358 respondents.
2. Measures
2.1 Dependent variables
2.1.1 Physical activity
In the present study, physical activity is assessed by measuring moderate-to-vigorous physical activity (MVPA). MVPA is defined in the HBSC questionnaire as “any activity that increases your heart rate and makes you get out of breath some of the time”. Examples such as dancing, swimming, or running are included in the questionnaire to illustrate what is meant by this definition. MVPA was assessed by asking the following question: “over the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day if you add up all the time you spent in physical activity”. A continuous variable was constructed with responses ranging from 0 to 7 days. Visual inspection of the histogram, Q-Q plot and boxplot showed that MVPA was approximately normally distributed. This MVPA measure has been validated and deemed reliable for assessing physical activity in young people (Biddle et al., 2011).
2.1.2 Screen time related sitting
Sedentary behaviors can be subdivided into screen-based and non-screen-based activities (Olds et al., 2010). Although non-screen-based activities constitute the highest proportion of overall sitting time, meta-analysis in an adult population has shown that screen-based activities represent a more serious health risk (Byun, Dowda, & Pate, 2012; Ekelund et al., 2016; O’Brien, Issartel, & Belton, 2018). Screen-based sedentary behaviors are therefore measured in the present study as screen time related sitting (STRS). STRS was assessed in relation to three different settings: TV use, computer use for game playing, and computer use for other purposes (e.g. homework, emailing).
To measure the time spentwatching TV during leisure time, participants were asked the following
question: ”How many hours a day, in your free time, do you usually spend watching TV, videos (including YouTube or similar services), DVDs, and other entertainment on a screen?”. The time spent playing computer games in participants’ leisure time was assessed by asking; “How many hours a day, in your free time, do you usually spend playing games on a computer, games console, tablet (like iPad), smartphone or other electronic device (not including moving or fitness games)?”. Computer use for other purposes in leisure time was measured by asking; “How many hours a day,
in your free time, do you usually spend using electronic devices such as computers, tablets (like
iPad) or smartphones for other purposes, for example, homework, emailing, tweeting, Facebook, chatting, surfing the internet?”. Response options were the same across the three different items. Participants were asked to select one option for week days and one option for weekend days.
Options ranged from “none at all” to “about 7 hours or more a day”. To represent time measured in the amount of hours spent on screen-based activities, the variables were recoded. The three screen time behaviors were summed for week and weekend days separately to represent the total amount of time spent on screen-based activities per day. To combine summed measurements from week days and weekend days into one continuous variable, screen time related sitting (STRS), a weighted average was calculated: ("#$%&''(')*×,).("#$%&''(*/0×1)
2 . Visual inspection of the
histogram, Q-Q plot and boxplot showed that STRS was approximately normally distributed. While caution is required when interpreting self-reported measures (Steene-Johannessen et al., 2016), several studies reported a modest yet acceptable reliability and validity of the HBSC screen-time related sitting items (Vereecken, Todd, Roberts, Mulvihill, & Maes, 2006; Bobakova et al., 2015).
2.2 Independent variables
2.2.1 Parental education
Parental education was used as SES measure. This was based on the participants’ self-reports. Response options were divided into five levels: never studied, primary school, secondary school, (applied) university and “don’t see/don’t have father/mother”. For the purpose of this study the parent with the highest educational level was selected to represent parental education. After
recoding, parental education comprised four categories. Missing cases (Nmissing = 1086) and ‘don’t
see/have father/mother’ were categorized as ‘missing’ and included in the analyses. The response options ‘never studied’ and ‘primary school’ were redefined as ‘lower parental education’, ‘secondary school’ as ‘intermediate parental education’ and ‘(applied) university’ was presented as a fourth category: higher education. There is much evidence to support the validity of the information provided by adolescents in regards to their parental education (Pilgrim & Blum, 2012).
2.2.2 Health literacy
The participants’ subjective HL was assessed by using the Health Literacy for School-Aged Children (HLSAC) instrument (O. Paakkari et al., 2016). Within the instrument the participants were asked to respond to ten items. These ten items included two items from five predetermined theoretical components: theoretical knowledge, practical knowledge, critical thinking, self-awareness and citizenship. Responses to the ten items ranged from 1 (not at all true) to 4 (absolutely true). A sum score was generated from the ten items to create a continuous variable. The HLSAC instrument has a high internal consistency (Cronbach’s α = 0.93). In addition, research has confirmed reliability of its use in the assessment of adolescent HL (Guo et al., 2018).
2.2.3 Control variables
Ethnicity, gender, age and self-rated health (SRH) were included in the analysis to control for potential confounding. These variables have been previously identified as being related to sedentary behavior and physical activity (Temmel & Rhodes, 2013; Herman, Hopman, & Sabiston, 2015) while also being associated with HL and parental education (only ethnicity and SRH) (Laaksonen et al., 2005; Protheroe et al., 2017; Blom et al., 2018). Ethnicity was recoded into a dummy variable: respondents reporting that they were born in Belgium were coded as 0, all other responses were coded as 1. Gender was also coded as a dummy variable: “boy” was coded as 1 and “girl” was coded as “0”. In measuring self-rated health, the HBSC questionnaire included four response options (excellent, good, fair, poor) to the question; “Would you say your health is …?”. Following the suggestion in Schnohr (2016), a cut-off was used to minimize ambiguity with “fair” health: poor and fair (coded 1) versus good and excellent health (coded 0). Self-rated health has been proven to be reliable indicator for general objective health (Cavallo et al., 2006).
3. Statistical analysis
Prior to the analyses, data cleaning and recoding of variables was performed in IBM SPSS® Statistics (version 25). The same software was used for bivariate analyses without control variables to confirm the interrelationships parental education, adolescent HL and both MVPA and STRS. In the main analyses, a multilevel approach was applied to account for clustering of students (N=9358) within schools (N=194). For each of the health behavior outcomes (STRS and MVPA), random intercept models were fitted by using MLwiN version 2.36. The equations can be found in appendix C. The analysis was constructed stepwise. Containing only the intercept, the null model was estimated. Next, in the first model, the relationship between HL and the health behavior outcomes was assessed. The second model estimated the relationship between parental education and the health behavior outcomes. Both HL and parental education were included in the third model for the purpose of examining whether HL may explain part of the relationship between parental education and health behaviors. All models were controlled for age, gender, ethnicity and SRH. To give an indication of the overall goodness-of-fit, the -2LogLikelihood was reported for each model. Lower values indicate a better fit. To facilitate the meaningful interpretation of the unstandardized regression coefficients, the continuous variables age and HL were centered around their grand mean. A P value of 0.05 was used to determine statistical significance.
Results
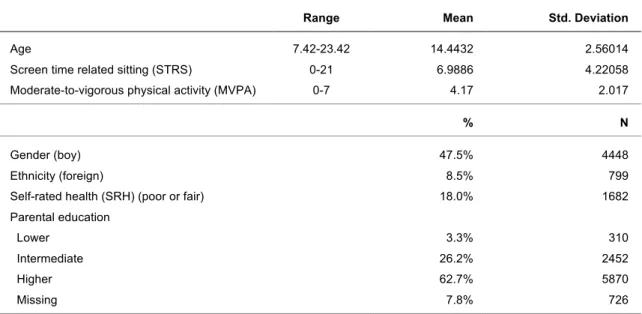
An overview of the descriptive statistics is provided in table 1. Out of all respondents 52.2% reported to be female and 91.5% reported to be Belgian. The age of the respondents ranged from 7.42 to 23.42 with a mean score of 14.44 (standard deviation 2.56). In regard to SRH, 18.0% of the respondents rated their health as fair or poor. The mean score for STRS is 6.99 (standard deviation 4.22) (range 0 – 21). MVPA had a mean score of 4.17 (standard deviation 2.02) (range 0 – 7). HL scores ranged from 2 to 40 with a mean score of 30.32 (standard deviation 5.29). Lower parental education was reported by 3.3% of the respondents. Intermediate (26.2%) and higher (62.7%) parental education were more frequently reported in comparison with lower parental education.
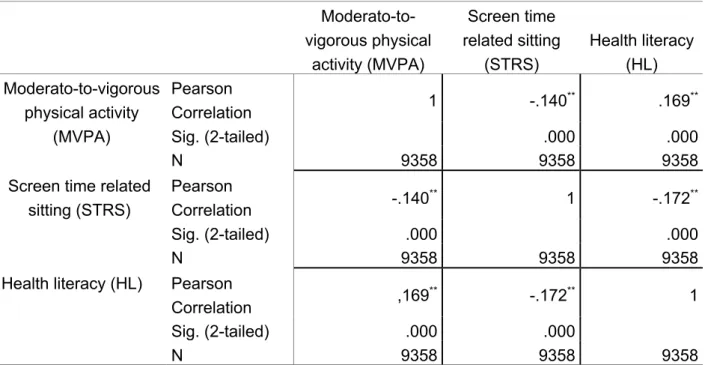
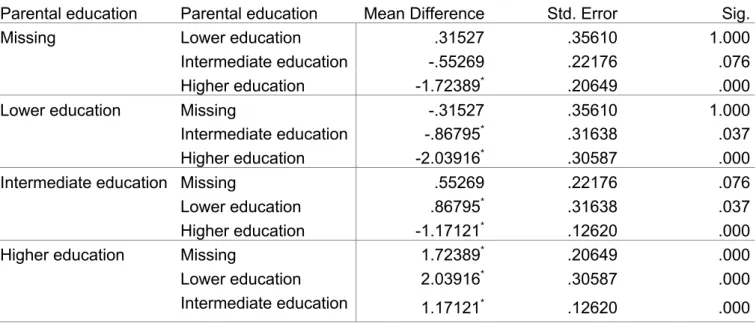
Bivariate analyses without control variables were significant (p < 0.001), confirming the existence of associations between HL, and both sedentary behavior and physical activity in adolescents. A one-way analysis of variance (ANOVA) showed significant differences in HL, physical activity and sedentary behavior between parental education groups (p < 0.001) in adolescents. More precisely, in regard to HL, post-hoc comparisons using the Bonferroni correction showed that average HL scores from respondents with lower parental education differed significantly from average HL scores from respondents with intermediate parental education (p < 0.05) and higher parental education (p < 0.001). Mean HL scores also differed significantly between respondents with intermediate parental education and higher parental education (p < 0.001). On average,
Table 1. Descriptive statistics on age, gender, ethnicity, self-rated health, parental
education, health literacy, STRS and MVPA (Nindividuals = 9358).
Range Mean Std. Deviation
Age 7.42-23.42 14.4432 2.56014
Screen time related sitting (STRS) 0-21 6.9886 4.22058
Moderate-to-vigorous physical activity (MVPA) 0-7 4.17 2.017
% N
Gender (boy) 47.5% 4448
Ethnicity (foreign) 8.5% 799
Self-rated health (SRH) (poor or fair) 18.0% 1682
Parental education
Lower 3.3% 310
Intermediate 26.2% 2452
Higher 62.7% 5870
respondents with lower parental education had a HL score of 29.18 (standard deviation 5.88). Respondents with intermediate parental education on average had a HL score of 29.66 (standard deviation 5.24). Respondents with higher parental education on average had the highest HL scores with a mean of 30.83 (standard deviation 30.83). The existence of significant interrelationships between parental education, HL and both physical activity and sedentary behavior in adolescents were hereby confirmed (data shown in appendix B).
1. Multilevel models
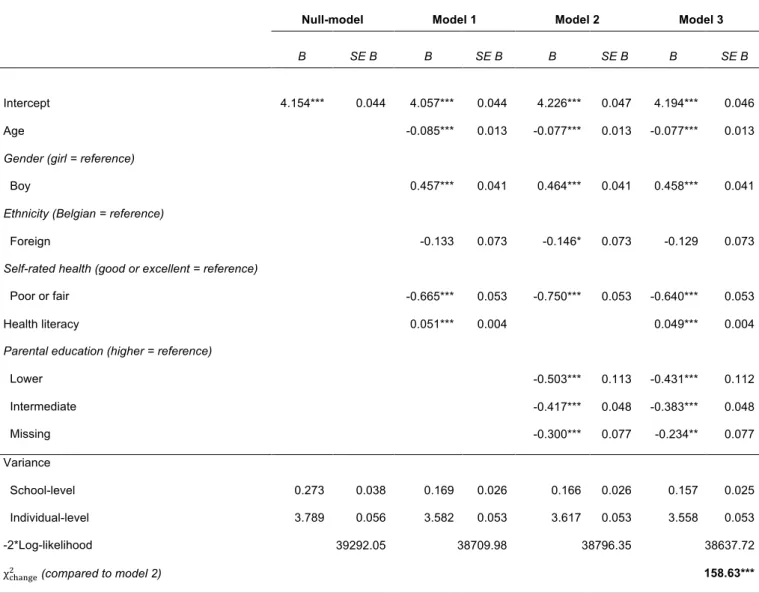
Table 2 and table 3 display the results of the multilevel analyses. Table 2 presents the results of four fitted random intercept models that predict STRS. The null model contains only the intercept for the prediction of STRS. Model 1 regressed STRS on the control variables and HL. The second model includes the control variables and parental education in predicting STRS. For model 3, HL was added to the previous model. Results of these four models, for the prediction of MVPA, are displayed in table 3. The tables display the unstandardized regression coefficients of the independent variables.
Across the three included models, for both the prediction of STRS and MVPA, the control variables age, gender and SRH were identified as significant predictors (p < 0.001). Higher age was significantly associated with more STRS and less MVPA, as was poor or fair SRH. Male students reported more STRS and more MVPA. In model 2, being foreign was associated with less MVPA, this result was significant at the 0.05 level. Across all other models, ethnicity was not identified as a significant predictor of either STRS or MVPA.
1.1 STRS and MVPA regressed on HL.
The multilevel analysis in model 1 revealed that HL was significantly associated with both MVPA and STRS. On average, students with higher HL scores reported less STRS (B= -0.097, p < 0.001) and more MVPA (B= 0.051, p < 0.001). The goodness-of-fit statistic, the deviance (-2*Log-likelihood), for model 1 was calculated as 51962.24 for STRS and 38709.98 for MVPA.
1.2 STRS and MVPA regressed on parental education.
In model 2, a significant relation was observed between parental education and STRS. In comparison to the higher parental education, both lower (B= 1.086, p < 0.001) and intermediate parental education (B= 0.724, p < 0.001) were associated with higher reports of STRS. The
deviance for this model was calculated as 52044.92. Less MVPA was observed in students reporting lower (B= -0.503, p < 0.001) and intermediate parental education (B= -0.417, p < 0.001) compared to higher parental education. The deviance statistic for the prediction of MVPA in model 2 was 38796.35.
1.3 STRS and MVPA regressed on parental education and HL.
In model 3, HL was added as an independent variable to the previous model. Lower levels of HL were significantly associated with more STRS (B= -0.093, p < 0.001), independent of parental education. In comparison to higher parental education, lower (B= 0.960, p < 0.001) and
Table 2. STRS regressed on age, gender, ethnicity, self-rated health, health literacy, and parental education
(Nindividuals = 9358; Nschools = 194)
Null model Model 1 Model 2 Model 3
B SE B B SE B B SE B B SE B
Intercept 7.068*** 0.130 9.572*** 0.265 6.309*** 0.120 6.364*** 0.117
Age 0.337*** 0.033 0.325*** 0.033 0.324*** 0.032
Gender (girl = reference)
Boy 0.695*** 0.084 0.681*** 0.084 0.695*** 0.083
Ethnicity (Belgian = reference)
Foreign -0.044 0.148 -0.016 0.149 -0.048 0.148
Self-rated health (good or excellent = reference)
Poor or fair 0.848*** 0.107 1.016*** 0.106 0.809*** 0.107
Health literacy -0.097*** 0.008 -0.093*** 0.008
Parental education (higher = reference)
Lower 1.086*** 0.229 0.960*** 0.228 Intermediate 0.724*** 0.098 0.666*** 0.098 Missing 0.622*** 0.157 0.504*** 0.156 Variance School-level 2.831 0.333 1.728 0.217 1.659 0.210 1.557 0.199 Individual-level 15.096 0.223 14.560 0.215 14.701 0.217 14.492 0.214 -2*Log-likelihood 52374.44 51962.24 52044.92 51903.27 χ45678%, (compared to model 2) 141.65***
N=9358; *p < .05, **p < .01, ***p<.001 (two tailed test).
Note. All continuous independent variables were centered around their grand mean. SE = Standard error
intermediate parental education (B= 0.666, p < 0.001) were both related to higher rates of STRS, independent of HL. The deviance was 51903.27 for model 3 predicting STRS. The likelihood ratio
test between model 3 and model 2 calculated a χ2-change of 141.65 (p < 0.001). Indicating that
adding HL to the second model resulted in a better fit of STRS.
Results from model 3 indicated that higher HL scores were associated with more MVPA (B= 0.049,
p < 0.001), independent of parental education. Respondents with lower (B= -0.431, p < 0.001) and
intermediate (B= -0.383, p < 0.001) parental education reported lower levels of MVPA compared
Table 3. MVPA regressed on age, gender, ethnicity, self-rated health, health literacy, and parental education
(Nindividuals = 9358; Nschools = 194)
Null-model Model 1 Model 2 Model 3
B SE B B SE B B SE B B SE B
Intercept 4.154*** 0.044 4.057*** 0.044 4.226*** 0.047 4.194*** 0.046
Age -0.085*** 0.013 -0.077*** 0.013 -0.077*** 0.013
Gender (girl = reference)
Boy 0.457*** 0.041 0.464*** 0.041 0.458*** 0.041
Ethnicity (Belgian = reference)
Foreign -0.133 0.073 -0.146* 0.073 -0.129 0.073
Self-rated health (good or excellent = reference)
Poor or fair -0.665*** 0.053 -0.750*** 0.053 -0.640*** 0.053
Health literacy 0.051*** 0.004 0.049*** 0.004
Parental education (higher = reference)
Lower -0.503*** 0.113 -0.431*** 0.112 Intermediate -0.417*** 0.048 -0.383*** 0.048 Missing -0.300*** 0.077 -0.234** 0.077 Variance School-level 0.273 0.038 0.169 0.026 0.166 0.026 0.157 0.025 Individual-level 3.789 0.056 3.582 0.053 3.617 0.053 3.558 0.053 -2*Log-likelihood 39292.05 38709.98 38796.35 38637.72 χ45678%, (compared to model 2) 158.63*** N=9358; *p < .05, **p < .01, ***p <.001 (two-tailed test).
Note. All continuous independent variables were centered around their grand mean. SE = Standard error
to respondents with higher parental education, independent of HL. For the prediction of MVPA, the goodness-of-fit statistic for model 3 resulted in a deviance of 38637.73. Compared to model 2, the
addition of HL as an independent variable offered a better fit of MVPA (χ,-change = 158.63; p <
0.001). More specifically, adding HL to the second model reduced the regression coefficients estimating the association of parental education. This was observed in the prediction of both MVPA and STRS. However, the associations between parental education and both MVPA and STRS remained significant after the addition of HL. This was the case for all levels of parental education, indicating that HL partly explains the association between parental education and MVPA and STRS.
Discussion
1. Adolescent health literacy and health behaviors
As hypothesized, an inverse relationship was demonstrated between HL and sedentary behavior. Students reporting lower HL tend to display more sedentary behavior than students with higher HL. This finding extends existing knowledge concerning health-related outcomes of HL. Previous studies examining associations between adolescent HL and health behaviors thus far have focused mainly on dietary behavior, physical activity, smoking and alcohol use. Sedentary behavior in adolescents, to the best of our knowledge has not been specifically examined in relation to HL. This may be due to the fact that sedentary behavior as a separate risk factor, independent of physical activity, has only been acknowledged in recent years (Sedentary Behaviour Research Network, 2012; Park et al., 2018)
Despite the fact that several studies report no significant associations between HL and physical activity in adolescents (Fleary et al., 2018), findings within this study provide evidence to the contrary. In line with few previous studies (Levin-Zamir et al., 2011), lower HL was significantly related to less physical activity in adolescents. Because existing research does not consistently report similar results, the findings in the present study do not necessarily support previous research. However, they do again highlight the need for more extensive research into HL’s link to physical activity and other adolescent health behaviors in general. This is especially true for sedentary behavior in adolescents.
2. SES and adolescent health behaviors
In examining the relationship between SES and sedentary behavior, the present study demonstrated that lower SES adolescents reported more sedentary behavior compared to higher SES adolescents. In addition, a positive relationship was found between SES and physical activity. Adolescents with lower SES reported lower levels of physical activity. SES correlates of sedentary behavior in adolescents have been subjected to research in the past. Previous research has shown that relationships between SES and sedentary behavior vary by domain of sedentary behavior (e.g. screen-based sedentary behavior), measure of SES and between high- and low-middle-income countries (Mielke et al., 2017). Studies measuring SES by parental education, in high-income countries and examining STRS, reported results similar to the findings in this study. The present study is limited to the measurement of screen-based activities when assessing sedentary behavior. As relationships between SES and sedentary behavior in adolescents may differ by domain of sedentary behavior, caution is required when making inferences on SES differences in sedentary behavior in general. Making inferences on the relationship between parental education or SES, and sedentary behavior, without distinguishing between screen-based and non-screen based activities, may not be valid. The concept of sedentary behavior has changed during the last decade and a consensus definition has not yet been established (Gibbs, Hergenroeder, Katzmarzyk, Lee, & Jakicic, 2015; Tremblay et al., 2017). The results presented within this study can be seen as a valuable addition to the growing amount of research that supports the further refinement of the concept of sedentary behavior.
Physical activity in adolescents has been related to SES in the past. However, this relationship has not been consistently described as significant across different studies. Further research is required to better understand SES differences in physical activity in adolescents (Hanson & Chen, 2007). One surprising finding relates to the control variable ethnicity. Only in regressing physical activity on parental education is ethnicity found to be a significant predictor. In all other models presented in this study, foreign status of adolescents is not significantly associated with physical activity or sedentary behavior. This contradicts previous research (Gordon-Larsen, McMurray, & Popkin, 1999; Brug et al., 2012). However, ethnicity as a control variable was not removed from the analyses.
3. Adolescent health literacy and socioeconomic differences in health behaviors
The findings in the current study confirm the hypothesis that HL partly explains socioeconomic differences in adolescent health behaviors. This is evident from the reduction of the regression coefficients of parental education after adding HL to the model. These results are similar to the findings of Friis et al. (2016) who identified HL as a mediator in the relationship between educational attainment as SES measure, and health behaviors in adults.
Within the present study, the addition of adolescent HL to the regression model attenuated the relationship between SES and the examined health behaviors. SES remained significantly related to both physical activity and sedentary behavior after taking into account adolescent HL. Therefore, this study suggests that adolescent HL contributes to the link between SES and both health behaviors although it does not offer a complete explanation. It is important to acknowledge that other factors related to SES and health behaviors among adolescents could be part of the mechanisms explaining the association between SES and health behaviors in adolescents (Pampel et al., 2010); Cocker et al., 2012; Cheng, Mendonça, Lucena, Rech, & Farias, 2018). For instance, in regard to physical activity as a health behavior outcome of SES in adolescents, environmental factors (e.g. cost, proximity, facilities and safety) as well as individual traits (e.g. esteem, self-efficacy) have been identified as potential mediators (Humbert et al., 2006; Veselska, Madarasova Geckova, Reijneveld, & van Dijk, 2011; Cocker et al., 2012). The present study adds adolescent HL to this limited list of possible mechanisms of socioeconomic differences in adolescent health behaviors. The findings in the current study, combined with the acknowledgement of other existing mechanisms, suggest that interventions addressing adolescent health behaviors to reduce socioeconomic inequalities in health require a multifaceted approach. The paucity of research exploring the mechanisms by which SES relates to health behaviors in adolescents (Cheng et al., 2018) needs to be addressed in future research.
4. Strengths and limitations
This study has some limitations. First, since the findings in this study were based on cross-sectional data, no conclusions on causation or temporality can be made. Second, data was collected by using standardized questionnaires (Inchley et al., 2018). As a result, measures for adolescent HL, physical activity and sedentary behavior were self-reported by the students. Although the instruments that were used to assess these factors have been described as adequately reliable (Inchley et al., 2018), possible response bias should be taken into account. Future research may
be strengthened by the use of objective measures for health behaviors. Third, it should be noted that associations between lower SES and negative health behaviors may be more likely when choosing parental education as an SES measure (Hanson & Chen, 2007). As adolescents transition into the independence of adulthood and spend less time at home, the use of parental SES measures may become less valid (Hanson & Chen, 2007). The current study does not take into account the moderating effects of age in examining the relationship between SES and health behaviors. Furthermore, other SES markers may provide different results depending on the health behavior that is being assessed. Future research can benefit from the use of multiple SES markers (e.g. Family Affluence Scale (FAS), perceived SES in comparison with others in immediate social network, parental occupation) (Hanson & Chen, 2007; Svedberg, Nygren, Staland-Nyman, & Nyholm, 2016). Fourth, the assessment of adolescent HL marks both a strength and a limitation of this study. HL was assessed by using the HLSAC instrument developed by O. Paakkari et al. (2016). The HLSAC instrument can be seen as an operationalization of HL defined as a learning outcome in schools (L. Paakkari & Paakkari, 2012). By defining HL as a learning outcome in school, the HLSAC instrument detaches HL from real-life actions and behaviors (Okan, Bauer, Pinheiro, et al., 2019). Furthermore, developmental characteristics that could influence health behaviors in adolescents are not considered in the theoretical framework that supports the HLSAC instrument (Fleary et al., 2018). Notwithstanding these arguments, the use of a HL measure specifically developed for adolescents marks a strength of this study. Researchers examining HL in adolescents rarely make use of instruments that are specifically developed for this target group (Fleary et al., 2018). This study therefore contributes to the body of evidence that supports the much-needed ongoing conceptual development of both HL in general and adolescent HL. Fifth, the HBSC study provides data on sedentary behavior by measuring time spent on screen-based activities. As such, no distinction is made between screen-based and non-screen based activities. Future research can benefit from a more complete assessment of sedentary behavior through the measurement of both screen-based and non-screen based activities.
Although this study provides evidence for the contribution of HL in socioeconomic differences in adolescent health behaviors, no mediation analysis was conducted. Therefore, no statements can be made about the size of the effect of SES on adolescent health behaviors through adolescent HL. Further research needs to address this issue by examining how much of the variance between SES and health behaviors can be accounted for by HL in adolescents.
The nested-structure in which the data was collected allowed for the use of multilevel analyses. By using multilevel analyses, the current study was able to control for cluster bias at the school level. In predicting sedentary behavior and physical activity respectively 15.79% and 6.72% of the variance can be explained at the school level. These results reflect the importance of taking into account schools as a contextual influence on health behaviors. Future studies should examine these contextual influences by taking into account different school-related characteristics in their analyses.
A key strength lies within the fact that this study investigated gaps in knowledge that had not been examined extensively before. These include adolescents as a target group, health behaviors (especially sedentary behavior) as outcomes and HL’s role in socioeconomic differences in health-related outcomes. More specifically, HL’s role in socioeconomic differences in adolescent health behaviors had not been previously addressed in research to the best of our knowledge.
Conclusions
This study has produced several meaningful findings. First, the present study demonstrated that there is a significant relationship between adolescent HL and health behaviors. Second, a significant association has been found between SES and health behaviors in adolescents. Lastly, this study has successfully shown that HL partly explains socioeconomic differences in health behaviors in adolescents. These findings confirm the hypotheses that were put forth.
Relevance for practice and recommendations
The findings in this study identify adolescent HL as a mechanism by which SES influences adolescent health behaviors. However, adolescent HL does not offer a complete explanation for socioeconomic differences in adolescent health behaviors. Tackling socioeconomic inequalities in health by addressing adolescent health behaviors therefore requires a multifaceted approach. This approach should include, but not be restricted to, interventions aimed at improving adolescent HL. Research regarding this subject is scarce and future studies need to examine adolescent HL’s role in socioeconomic differences in other health behaviors as well (e.g. smoking, dietary behavior, alcohol use). Additionally, future studies that examine HL’s role in the relationship between SES and adolescent health behaviors should include different SES measures. In general, future
research can benefit from more extensive research into the concepts of HL and adolescent HL as well as sedentary behavior. Furthermore, the multilevel approach used in this study identified schools as a contextual influence on both sedentary behavior and physical activity. More extensive and explanatory research is required to examine the influence at the school-level.
References
Adler, N. E., & Newman, K. (2002). Socioeconomic Disparities In Health: Pathways And Policies.
Health Affairs, 21(2), 60–76. https://doi.org/10.1377/hlthaff.21.2.60
Antonovsky, A. (1967). Social class, life expectancy and overall mortality. The Milbank Memorial
Fund Quarterly, 45(2), 31–73. https://doi.org/10.2307/3348839
Australia. Department of Health, H., Services, C., Nutbeam, D., Health, U. of S. D. of P., Nutbeam, D., Wise, M., Bauman, A., Harris, E., & Leeder, S. (1993). Goals and targets for Australia’s
health in the year 2000 and beyond: Report prepared for the Commonwealth Department of Health, Housing & Community Services ([Rev.]). Sydney : Public Health Dept., University
of Sydney. https://trove.nla.gov.au/version/39872272
Baker, D. W., Wolf, M. S., Feinglass, J., Thompson, J. A., Gazmararian, J. A., & Huang, J. (2007). Health Literacy and Mortality Among Elderly Persons. Archives of Internal Medicine,
167(14), 1503–1509. https://doi.org/10.1001/archinte.167.14.1503
Bennett, I. M., Chen, J., Soroui, J. S., & White, S. (2009). The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Annals
of Family Medicine, 7(3), 204–211. https://doi.org/10.1370/afm.940
Berkman, N. D., Sheridan, S. L., Donahue, K. E., Halpern, D. J., & Crotty, K. (2011). Low Health Literacy and Health Outcomes: An Updated Systematic Review. Annals of Internal
Medicine, 155(2), 97. https://doi.org/10.7326/0003-4819-155-2-201107190-00005
Biddle, S. J. H., Gorely, T., Pearson, N., & Bull, F. C. (2011). An assessment of self-reported physical activity instruments in young people for population surveillance: Project ALPHA.
The International Journal of Behavioral Nutrition and Physical Activity, 8, 1.
https://doi.org/10.1186/1479-5868-8-1
Blom, I. M., Cohen, E. S., Eshuis, L. V., Woudstra, A. J., Snijder, M. B., Kunst, A. E., & Fransen, M. P. (2018). Ethnic Differences in Health Literacy Among Young Adults in Amsterdam.
Health Literacy Research and Practice, 2(4), e192–e204. https://doi.org/10.3928/24748307-20180926-01
Bobakova, D., Hamrik, Z., Badura, P., Sigmundova, D., Nalecz, H., & Kalman, M. (2015). Test-retest reliability of selected physical activity and sedentary behaviour HBSC items in the Czech Republic, Slovakia and Poland. International Journal of Public Health, 60(1), 59–67. https://doi.org/10.1007/s00038-014-0628-9
Bröder, J., Okan, O., Bauer, U., Bruland, D., Schlupp, S., Bollweg, T. M., Saboga-Nunes, L., Bond, E., Sørensen, K., Bitzer, E.-M., Jordan, S., Domanska, O., Firnges, C., Carvalho, G. S.,