FEASIBILITY AND EFFECTIVENESS OF A
GAMING MAT IN THE REHABILITATION
OF CHILDREN WITH COORDINATION
AND/ OR BALANCE PROBLEMS
A PRELIMINARY STUDY
01407765
Sarah Cornil
01313540
Charlotte Van Den Hende
01410469Laura Van Renterghem
Supervisors: Prof. Dr. Hilde Van Waelvelde, Arno Penders
A dissertation submitted to Ghent University in partial fulfilment of the requirements for the degree of Master in Rehabilitation Sciences and Physiotherapy
FEASIBILITY AND EFFECTIVENESS OF A
GAMING MAT IN THE REHABILITATION
OF CHILDREN WITH COORDINATION
AND/ OR BALANCE PROBLEMS
A PRELIMINARY STUDY
01407765
Sarah Cornil
01313540
Charlotte Van Den Hende
01410469Laura Van Renterghem
Supervisors: Prof. Dr. Hilde Van Waelvelde, Arno Penders
A dissertation submitted to Ghent University in partial fulfilment of the requirements for the degree of Master in Rehabilitation Sciences and Physiotherapy
Acknowledgement
We are finalizing our thesis by writing this word of gratitude. It was a period in which we learned a lot, scientifically, practically, but also personally. We would like to acknowledge our appreciation towards the people who made it possible to write this thesis by their support and cooperation. First of all, we want to express our gratitude to our promoter Prof. Dr. Hilde Van Waelvelde for all the time and energy she spent during the two years of our master thesis. She guided us not only in terms of content, but also in terms of structure. Furthermore, she was always open to our questions and gave us a lot of practical help and constructive feedback.
Secondly, we want to thank Creative Therapy and in particular our co-promoter Arno Penders. Especially for the information and advice according to the gaming mat ‘Matti®’. We also want to emphasize our appreciation to Sébastien Michiels, Jamil Joundi and Ward Dehairs for their time to come to the school and rehabilitation center to fix the mat when facing technical issues. Thirdly, we want to thank Julie Van Winghem, Inge Mouton, Piet Verdegem, Astrid Verdegem,
Ann Declercq and Alien Schoenaers, the physiotherapists from Sint-Lievenspoort and CAR Klimop, for participating in this study. We want to express our sincere appreciation for the time, energy, creativity, space and practical help to ensure us to test and give therapy. We are also very grateful to the parents from our participants and the children with their enthusiasm, for their participation in this research.
Fourthly, we are grateful for the department of Physical Therapy and Rehabilitation Sciences of Ghent University to give us permission to conduct this study.
Last but not least, we want to thank our parents and friends for the support and the encouragements during our study process and in the realization of this thesis.
Tabel of contents
Acknowledgement ... 5
List of figures and tables ... 8
Abbreviations ... 9
Literature study ... 11
Abstract and key words (English) ... 12
Abstract and key words (Nederlands)... 13
Introduction ... 14 Method ... 17 Study design ... 17 Participants ... 17 Outcome measures ... 17 Intervention: ... 20 Statistical analysis ... 21 Results ... 22 Participants ... 22 Balance ... 22 Motivation ... 25 Qualitative observations ... 26 Discussion ... 27
Most important results ... 27
Future protocol... 31
Conclusion ... 32
References ... 33
Abstract (lekentaal) ... 37
Appendix ... 46
Appendix 1: Questionnaire IMI balance circuit ... 46
Appendix 2: Questionnaire IMI Matti® ... 47
Appendix 3: Thermometer ... 48
List of figures and tables
Tables:
Table 1: Balance items of the M-ABC-2-NL Table 2: Items of the KTK-NL
Table 3: Age and gender of the participants Table 4: Total score of the IMI
Figures:
Figure 1: Protocol
Figure 2: Box-and-wisker plot of the results of the M-ABC-2-NL
Figure 3: Box-and-wisker plot of the results of the KTK-NL: backwards balancing Figure 4: Box-and-wisker plot of the results of the KTK-NL: sideways jumping Figure 5: Average scores of the IMI
9
Abbreviations
↑ Increase
↓ Decrease
= Remains the same χ2 Chi-squared
ADHD Attention Deficit Hyperactivity Disorder ASD Autism Spectrum Disorder
BB Balance Beam BC Balance Circuit
CAR Center for Ambulatory Rehabilitation CoP Center of Pressure
CP Cerebral Palsy
CET Cognitive Evaluation Theory
DCD Developmental Coordination Disorder DLD Developmental Language Disorder e.g. example given, for example etc. etcetera
FASD Fetal Alcohol Spectrum Disorders IMI Intrinsic Motivation Inventory IQ Intelligence Quotient
IQR Interquartile Range
KTK-NL Körperkoordinationstest Für Kinder - Nederlandse vertaling LJ Lateral Jumps
M-ABC Movement Assessment Battery for Children
M-ABC-2 Movement Assessment Battery for Children second edition
10
MQ Motor Quotient P Significance Q-Q Quantile-Quantile
RCT Randomized Controlled Trial SD Standard Deviation
SDT Self-Determination Theory SJ Single-lever Jumps
SPSS Statistical Package for the Social Sciences
STABEL Sensorimotor Training to Affect Balance, Engagement and Learning
T Testing
T0 Test at baseline
T1 Test after three weeks of balance circuit intervention T2 Test after three weeks of intervention with Matti® TP Transfers on Platforms
11
12
Abstract and key words (English)
Background: Throughout the last decade, the use of Active Video Games (AVG) in the rehabilitation of children has become more common with evidence for their use in achieving rehabilitation goals. Besides, AVG are assumed to improve motivation and compliance. Matti® is a gaming mat designed by Creative Therapy for use in physical rehabilitation.
Objectives: The aim of the present study was to evaluate the effectiveness of Matti® compared to a conventional balance circuit at improving balance and motivation in children with mild coordination and balance problems.
Study design: A feasibility study combined with a pilot study, to evaluate effectiveness of the gaming mat, in order to enhance balance and motivation.
Methods: Twelve children (eight boys and four girls), aged between seven and 11 years old, with balance problems participated. All children began with three weeks of intervention on a balance circuit, followed by another three weeks of intervention on the gaming mat 'Matti®'. One baseline assessment, one assessment after three weeks and one assessment after six weeks were performed for balance using the Movement Assessment Battery for Children – second edition – Nederlandse vertaling (M-ABC-2-NL) and the Körperkoordinationstest für Kinder - Nederlandse vertaling (KTK-NL). To determine motivation, children had to complete the Intrinsic Motivation Inventory (IMI) after each therapeutic session.
Results: The balance exercises on Matti® with the different adopted games were feasible to be performed by the children. No significant improvement in scores of the subtests of the M-ABC-2-NL and the KTK-M-ABC-2-NL was found between baseline, three weeks or six weeks. Nor was there any statistical change in motivation.
Conclusion: Matti® seems to be a promising device to perform balance training in children. Effectiveness in rehabilitation of balance or enhancement of motivation and participation has yet to be shown.
13
Abstract and key words (Nederlands)
Achtergrond: Doorheen de laatste decennia is het gebruik van Active Video Games (AVG) in de revalidatie bij kinderen toegenomen en onderzoek suggereert mogelijks effectiviteit. AVG worden verondersteld de motivatie te verhogen. De gaming mat ‘Matti®‘ werd ontworpen door Creative Therapy met als doel om geïntegreerd te worden in fysische revalidatie.
Doelstellingen: Het doel van de huidige studie was om de effectiviteit van Matti® te evalueren, in vergelijking met een conventioneel evenwichtsparcours, om het evenwicht en de motivatie te verbeteren bij kinderen met milde coördinatie- en evenwichtsstoornissen.
Studie design: Een haalbaarheidsstudie gecombineerd met een piloot studie, om de effectiviteit te evalueren van de gaming mat, met als doel het evenwicht en de motivatie te verbeteren. Methode: Twaalf kinderen (acht jongens en vier meisjes tussen zeven en 11 jaar) met evenwichtsproblemen, namen deel aan deze studie. Alle kinderen startten met een interventie van drie weken met een evenwichtsparcours, gevolgd door een interventie van opnieuw drie weken met de mat. De Movement Assessment Battery for Children – 2 (M-ABC-2-NL) en de Körperkoordinationstest für Kinder (KTK-NL) werden gebruikt om het evenwicht te testen bij het begin, na drie weken en na zes weken interventie. Om de mate van motivatie na te gaan, werd aan de kinderen gevraagd om na elke interventie de Intrinsic Motivation Inventory (IMI) in te vullen.
Resultaten: Het was haalbaar om evenwichtsoefeningen op Matti®, met de verschillende aangepaste spelletjes, door kinderen te laten uitvoeren. Er werd geen significante verbetering gevonden van de scores op de subtesten van de M-ABC-2-NL en de KTK-NL over het verloop van de drie testmomenten. Dit geldt ook voor de IMI.
Conclusie: Matti® lijkt een veelbelovend middel om te werken aan evenwicht bij kinderen. De effectiviteit moet nog bewezen worden zowel voor het verbeteren van evenwicht, als voor het verbeteren van motivatie.
14
Introduction
Research has been conducted into the effect of gaming devices on balance rehabilitation of children with coordination disorders. Approximately 73 to 87% of children with poor motor performance have problems with balance (1). This implies that those children have problems with maintaining an upright position and with keeping the centre of gravity within the limits of support (1). Balance problems are one of the most frequently reported problems in Developmental Coordination Disorder (DCD). DCD is a common neurodevelopmental disorder, affecting 1,8 to 4% of school aged children (2). Affected children may experience difficulties in the planning, organization and/or execution of movements resulting in delays in the acquisition of fine and gross motor skills (3). Balance difficulties in children are not limited to those with a diagnosis of DCD and are also present in conditions such as Autism Spectrum Disorder (ASD), Attention Deficit and Hyperactivity Disorder (ADHD) and Cerebral Palsy (CP) (4). Children may encounter problems with a range of motor tasks such as running, dressing and writing (5). Motor deficits are particularly apparent in difficult, unexpected or novel situations (6). Difficulties in these skills can make it harder for children to be socially included, for example in team sports (7), or to fulfil the child's potential in school where an inability to record information quickly and neatly can be mistaken for laziness or low academic ability. This often leads to harmful secondary consequences such as poor academic achievement, low self-esteem (2, 7-9), reduced physical activity participation (10) and obesity (8).
Over the last decade, the use of Active Video Games (AVG), also called exergames, has become more common in the rehabilitation of children. Recent research suggests that the use of virtual reality (VR) systems may be beneficial as an intervention tool for motor deficits in a variety of situations (4). VR utilizes interactive simulations created with computer hardware and software, providing opportunities to interact and manipulate virtual objects in real-time, in a multidimensional and multisensory virtual environment (11). An example of a VR device is the Nintendo Wii, which is frequently used in combination with a balance board. Several studies found positive results by including Wii training into physiotherapy interventions in children with DCD (12-15). Similar results were found with Sony’s PlayStation 2 (16), the Xbox (17) and lesser known devices such as Sensorimotor Training to Affect Balance, Engagement and Learning (STABEL) (18), the Grail system (19) and the iBalance system (20). It is believed active games improve balance in motor impaired children by providing immediate feedback (15). Almost all populations studied to date describe an improvement in balance as a result of exergames, although further evidence is required to ensure these results reliable across multiple populations.
15 Exergames not only enhance motor performance, but are also stated to enhance motivation (21). Motivation is essential in any aspect of behavioural change (22). Motivation is considered an important prerequisite to successful rehabilitation (21). Adding game elements to a rehabilitation program is expected to enhance motivation, though limited research currently exists. There are preliminary indications that children who are more motivated by providing new opportunities and more variety to rehabilitation paradigms, such as VR or a robotic assistant, have a better rehabilitation outcome (23). It has the ability to fulfil the basic psychological needs of autonomy, belonging and competence described by the Self-Determination Theory (SDT) (24). This theory views internalization as the process of transforming external regulations into internal regulations and, when the process functions optimally, integrating those regulations into the sense of one self (24, 25). The theory uses the concepts of introjection and integration to describe two different types of internalization that result in different qualities of regulation. Introjection refers to partial or suboptimal internalization resulting in internally controlling regulation. Integration refers to optimal internalization resulting in self-determined behaviour (26). Another theory that directly relates to intrinsic motivation is the Cognitive Evaluation Theory (CET) (27). Intrinsic motivation is “based on the satisfactions of behaving ‘for its own sake’ (28). If the situational context, e.g. playing exergames on a device, promotes the three basic needs (autonomy, belonging and competence), then the natural behaviour of a person is more likely to be motivated (22). The need for self-competence can be fulfilled by varying game difficulty and player skills and by providing instant feedback on performance to ensure the player is challenged but tasks are achievable (29). Gaming devices, e.g. the Nintendo Wii, use a hand held controller and therefore cannot guarantee that the expected full-body movements are being used by the child (30). Creative Therapy, a team existing of engineers, game designers and developers, designed a gaming mat named 'Matti®' in collaboration with academic partners, physiotherapists and occupational therapists. Matti® has shown its feasibility to be used in a real therapy setting for rehabilitation of children with DCD (4). Matti® allows therapists to develop tailored therapy sessions using exergames to challenge specific patient deficits. Furthermore, the online Creative Therapy Platform helps therapists to follow the progress of their patients and adapt the therapy to the specific needs of the patient (4, 21). It is expected that the gaming mat can be used as a supporting device to give therapy and to motivate children at the same time (4), increasing patient enjoyment of rehabilitation. The Intrinsic Motivation Questionnaire (IMI), a questionnaire to quantify motivation, is among the most frequently used questionnaires in the context of sports and physical education (27) and will be implemented in this study.
16 Research has indicated that exergames can be useful to improve balance, not only beneficial for children with DCD, but also for those with other medical conditions or lower levels of physical fitness (12, 16-18, 20, 21, 31-38). The exergames do not only influence balance, but also motivation. To scientifically confirm these statements, more research is needed. Therefore, the aim of this pilot study is to determine if the gaming mat 'Matti®' can improve the balance in children and to determine if a difference in motivation exists between therapy on Matti® and conventional balance therapy.
17
Method
Study design
A feasibility study combined with a pilot study to evaluate effectiveness of the gaming mat in order to enhance balance and motivation. Ethical approval for this study was obtained from the ethical commission of the University of Ghent. Written informed consent was obtained from the parents of the children who participated in this study.
Participants
Two Centers for Ambulatory Rehabilitation (CAR), “CAR Klimop” and “CAR Impuls”, and one school for special education type 7 and 9, “Sint Lievenspoort”, were contacted by email and phone between July and September 2019. Inclusion criteria for the study were: (1) children aged between seven and 16 years old; (2) with an Intelligence Quotient (IQ) above 70; (3) who receive physiotherapy for mild coordination problems. Exclusion criteria were: (1) severe neuromotor disabilities (e.g. CP, severe orthopedic problems, etc.) that would make it impossible to undertake exercises on the mat. The parents of the participants were required to sign informed consent forms prior to the child commencing participation in this study.
Outcome measures
M-ABC 2-NL:
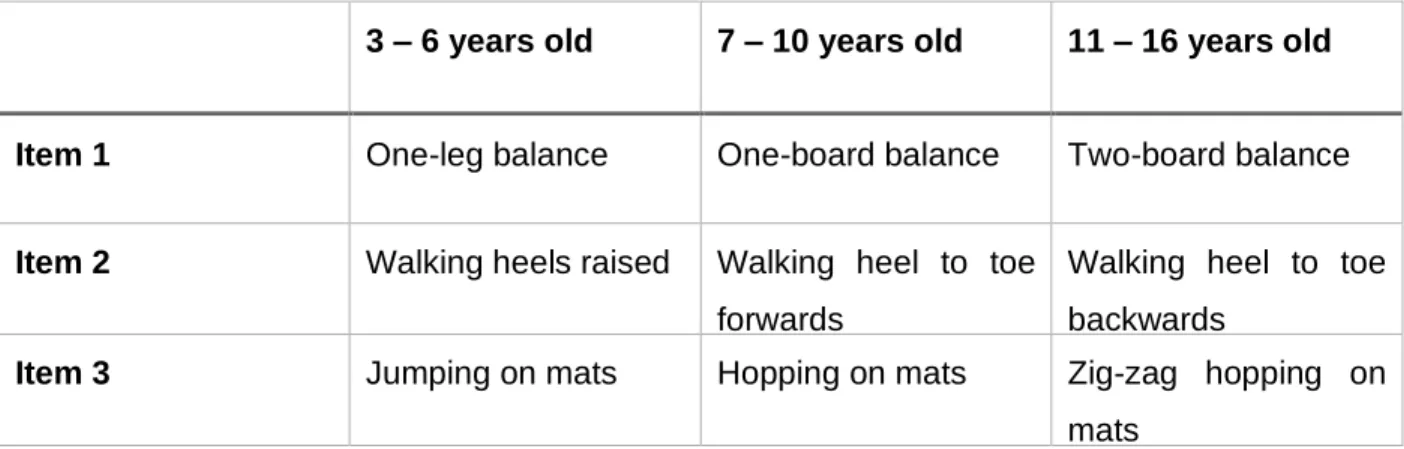
The M-ABC-2-NL is the Dutch translation of the Movement Assessment Battery for Children – second edition (M-ABC-2), a test of motor impairment that focusses on the identification and description of impairments in motor function for children aged between three and 16 years old. The test is divided in three age bands: three-six years old, seven-10 years old and 11-16 years old. The test is comprised of eight item, grouped into three motor skills sets; manual dexterity, ball skills and balance (39). This study only used the three items that correlate to balance skills (Table 1).
The M-ABC-2-NL was assessed for each participant at baseline, following three weeks of conventional balance therapy and following three weeks of intervention with the gaming mat. For the second test assessment, some of the participants were tested on the same day as their last intervention session of the balance circuit, while others were tested at a subsequent session prior to the intervention with Matti®. Test scores of the participants were converted to percentile scores and standardised scores for the age band of each participant. The balance standardised scores were used for statistical analyses of the balance outcomes.
18 There is extensive data demonstrating the validity of the first edition of the Movement Assessment Battery for Children (M-ABC), however this information cannot be generalised to the second edition of the M-ABC-2, as the two versions differ greatly (39). The guidelines for the M-ABC-2 report that the content of the M-ABC-2 is representative for the component desired to measure (40). Studies have shown a reasonable test-retest reliability for the M-ABC-2 (39), however research on the validity and reliability of this measure is limited. Yet it is greatly used in research, which makes it easy to compare scientific literature to this study.
3 – 6 years old 7 – 10 years old 11 – 16 years old
Item 1 One-leg balance One-board balance Two-board balance
Item 2 Walking heels raised Walking heel to toe forwards
Walking heel to toe backwards
Item 3 Jumping on mats Hopping on mats Zig-zag hopping on mats
Table 1: Balance items of the M-ABC-2-NL
KTK-NL:
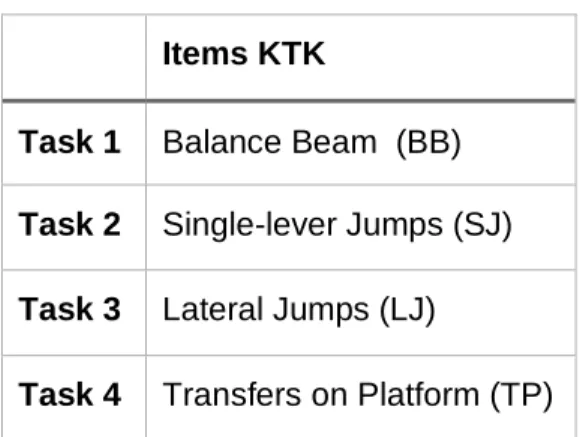
The Körperkoordinationstest für Kinder-Nederlandse vertaling (KTK-NL) is a test to assess gross motor coordination. It consists of four tasks, however this study only utilised tasks one and three (Table 2) to avoid exceeding the timeframe. The test is suitable for children between five and 15 years old with motor and/or intellectual disabilities and has been used to calculate normative data for 2831 Flemish children (41).
The KTK-NL tests were conducted at the same time as the tests of the M-ABC-2-NL; at baseline, following three weeks of conventional balance therapy and following three weeks of intervention with the gaming mat to detect an evolution in balance. The scores of the participants were converted into an age- and gender-related motor quotient (MQ).
19 The guideline of the KTK-NL declare that the test-retest reliability of the tasks separately are: BB 0.80 ; SJ 0.96 ; LJ 0.95 and TP 0.94, with the KTK-NL having a total reliability of 0.97. However, a factor analysis showed that the KTK-NL only measures general dynamic coordination and body control (41).
Intrinsic motivation inventory (IMI)
The IMI is a multidimensional measurement, invented by Ryan and colleges (27, 42), which consists of 45 items divided in seven subscales (43). The IMI aims to assess intrinsic motivation and the contributing factors that underly motivation (43).
The complete questionnaire is rarely used, with relevant subscales and items being utilised individually. It has been assumed that the omission of one subscale has no negative influence on the remaining factors. Shorter versions of each subscale have been used without change to the intrinsic consistence, indicating the ability for some items to be eliminated as required (43). An acceptable validity and reliability for the use of the IMI in competitive sport conditions has been demonstrated (44). Tsigilis and Theodosiou (2003) also found a Greek version of the scale to be reliable. Moreover, the IMI is assumed to be a temporal stable measure (45). This study excluded the original IMI subscales of perceived choice and relatedness as they did not apply to the study design. A 30-question questionnaire remained, which can be found in Appendix 1 for the balance circuit and in Appendix 2 for Matti®. The questionnaire consisted of normal questions, reversed questions and questions which needed to be answered with one word or sentence. The order of the questions was randomised.
Items KTK
Task 1 Balance Beam (BB) Task 2 Single-lever Jumps (SJ) Task 3 Lateral Jumps (LJ)
Task 4 Transfers on Platform (TP)
fhf(ggggj((TP)(TP)
20 The subscales that were used in this research were the 'interest/ enjoyment', 'perceived competence', 'pressure/ tension', 'effort/ importance' and 'value/ usefulness'. The 'interest/ enjoyment' subscale is considered the most direct self-report measure of intrinsic motivation by assessing the inherent joy of participants while performing an activity. The 'perceived competence' subscale is a positive predictor of intrinsic motivation and is related to the SDT. It measures how productive individuals feel when they are performing an activity. The 'pressure/ tension' subscale is a negative predictor of intrinsic motivation due to the evaluation of the pressure that participants feel to succeed a task. The 'effort/importance' subscale assesses the involvement of the participants. The 'value/usefulness' subscale assumes that people internalize and develop more self-regulatory activities when an activity is considered as valuable and useful for them (46).
After every training session, participants were required to score every item on a Likert scale going from 'one' (completely disagree) to 'seven' (completely agree). A colourful thermometer was used to visualise this scale (Appendix 3). This allows to calculate an average score per subscale and a total score, which is the summation of all the subscales (43). For the balance circuit and for Matti® an average of the three test scores of the IMI is made, so both scores could be compared. Participants were advised that if an item was unclear, they could ask for an explanation. If a researcher was unsure if the child understood an item, he or she was asked to summarise the content of that item to ensure the questions were interpreted correctly.
Intervention:
The gaming mat intervention consisted of games that the children could play on Matti® to improve balance. The intervention tool ‘Matti®’ is a mat of 1,5 m2 provided with pressure sensors which can be used to play a game via a computer and a screen in front of the child. Software with games were connected to Matti®, which registered the activity of the child. There were six different Matti® games that the participants could choose from. The first game was 'Whack-a-light', where the children had to jump from one light to another. The second game was 'The orchestra', where the children had to shift their weight to keep their center of pressure (CoP) in the middle of a moving circle. The third game was 'Simon says', where the children had to remember a sequence of colors and then jump from color to color in the right order. The fourth game was called 'Twister', where the children could play a 'twister by Creative Therapy' style game on the mat. The fifth game was 'Balance beam', where they had to walk on a line from one point to another without losing their balance. The last game was called 'Avoid the monster'. Here the participants had to run away or jump over a monster that was moving around on the mat. These games were meant
21 to improve static and dynamic balance. Each week, the participants played a selection of these games three times for four minutes in one session, with four minutes of rest in between. Each session, the children chose three games that they wanted to play.
The conventional balance therapy consisted of 20 minutes of balance circuit training. One session took place each week. A balance circuit, comprising of three sets of four minutes of exercises for static and dynamic balance, was performed with four minutes rest between sets.
In this study the participants received six weeks of continuous intervention. The first three weeks consisted of the conventional balance therapy, while the last three weeks consisted of the gaming mat intervention (Figure 1). The participants were assessed by the M-ABC-2-NL and the KTK-NL at baseline, after the conventional balance therapy and after the gaming mat intervention. The therapy and assessment took place in the rehabilitation center and the school. They were overseen by the researchers and were not blinded.
Statistical analysis
Statistical Package for the Social Sciences (SPSS) statistics 26 was used for data analysis. The normality of the data distribution was evaluated by the use of a Shapiro-Wilk test, a histogram and Quantile-Quantile (Q-Q) plots. Based on these outcomes, non-parametric statistical tests were chosen. Median and Interquartile Range (IQR) were used in descriptive statistics for balance results (Figure 2, 3 and 4). A Friedman test was used to compare the results on the M-ABC-2-NL, the KTK-NL and the IMI. The outcome of the balance tests was compared at baseline, after the conventional balance therapy and after the intervention with Matti®. The average outcome of the IMI after conventional therapy was compared to the average of the intervention with Matti®. Additionally, the three scores of the IMI after each intervention on Matti® were compared to assess whether the motivation attenuated. Significance (P) < 0,05 was determined as statistically significant.
22
Results
Participants
Fifteen children initially enrolled in this study. Three children dropped out due to lost to follow-up. Twelve children (eight boys and four girls) with the age between seven and 11 years old remained (Table 1). Six children were recruited from the school 'Sint Lievenspoort' and six children from rehabilitation centre for children 'CAR Klimop'. Five children had a diagnosis of Autism Spectrum Disorder (ASS), one child had a global developmental delay, one child had a brain injury, one child had a diagnose of Developmental Language Disorder (DLD) and four children had a diagnosis of both DLD and DCD. All of them had mild coordination problems. Due to health problems of participants, technical problems with Matti® and time-management issues there is missing data. Gender Total Male Female Age (years) 7y 2 0 2 8y 3 0 3 9y 1 2 3 10y 1 1 2 11y 1 1 2 Total 8 4 12
Table 3: Age and gender of the participants
Balance
As the data was not normally distributed, a non-parametric statistical Friedman test was chosen to evaluate the significance between outcome measures.
23 Descriptive statistics for balance component standard scores of the M-ABC-2-NL and the motor quotients of the backwards balancing (BB) and sideways jumping (SJ) of the KTK-NL for the first, second and third examination can be found in Appendix 4.
The distributions of the component standard scores for the M-ABC-2-NL and motor quotients for the KTK-NL are represented using box-and-whisker plots (Figure 2, 3 and 4).
Figure 2: Box-and-wisker plot of the results of the Figure 3: Box-and-wisker plot of the results of the M-ABC-2-NL KTK-NL: Sideways Jumping
Figure 4: Box-and-wisker plot of the results of the KTK-NL: Backwards Balancing
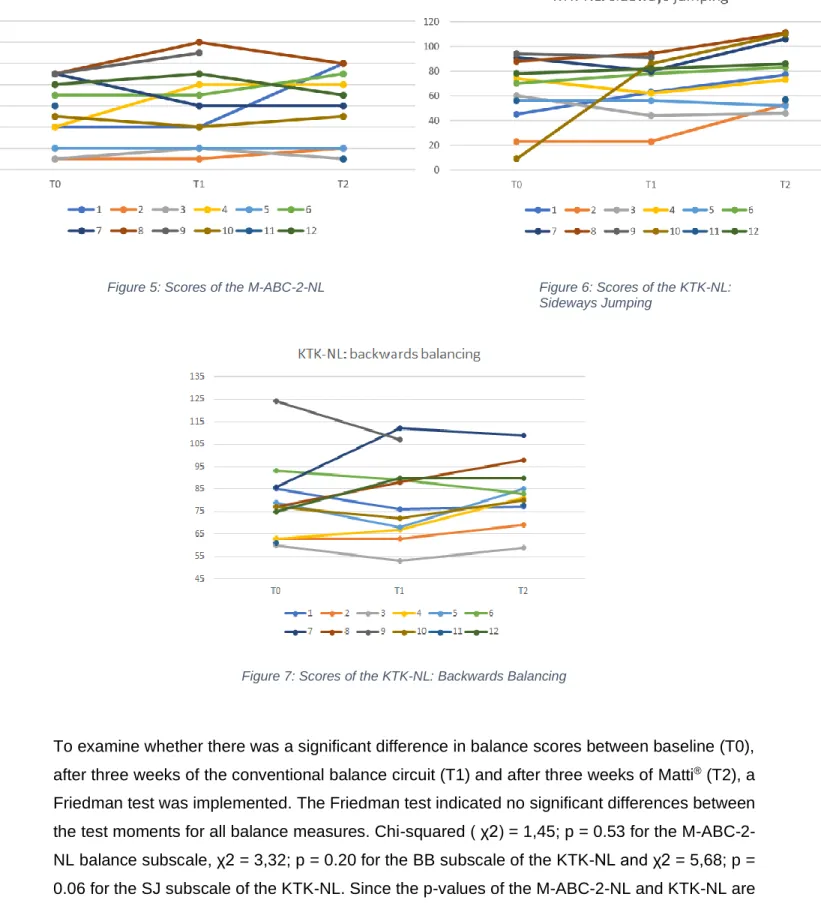
The subscores on balance for each child for every outcome measure (M-ABC-2-NL, KTK-NL: SJ and KTK-NL: BB) and for each test moment (baseline (T0), after three weeks of the conventional balance circuit intervention (T1) and after three weeks of the intervention with Matti® (T2)) can be found in figure 5, 6 and 7, respectively.
24
Figure 5: Scores of the M-ABC-2-NL Figure 6: Scores of the KTK-NL: Sideways Jumping
Figure 7: Scores of the KTK-NL: Backwards Balancing
To examine whether there was a significant difference in balance scores between baseline (T0), after three weeks of the conventional balance circuit (T1) and after three weeks of Matti® (T2), a Friedman test was implemented. The Friedman test indicated no significant differences between the test moments for all balance measures. Chi-squared ( χ2) = 1,45; p = 0.53 for the M-ABC-2-NL balance subscale, χ2 = 3,32; p = 0.20 for the BB subscale of the KTK-M-ABC-2-NL and χ2 = 5,68; p = 0.06 for the SJ subscale of the KTK-NL. Since the p-values of the M-ABC-2-NL and KTK-NL are higher than 0,05, the results are non-significant.
25
Motivation
The results of the IMI are individually reported in Table 4.
Child Balance circuit 1 Balance circuit 2 Balance circuit 3
Matti® 1 Matti® 2 Matti® 3
1 27,91 27,73 27,73 28,14 27,54 2 25,55 21,4 30,02 22,44 27,6 3 29,96 23,66 4 31,4 26,24 5 31,6 6 25,96 23,98 27,83 7 31,4 32,6 32,2 30,9 30,74 32,94 8 29,27 32,69 32,15 29,98 27,82 9 28,08 32,6 31,4 31,4 10 25,34 29,81 27,67 33,4 28,58 11 29 27,72 31,4 28,24 12 28,16 27,87 28,58 26,56
Table 4: Total score on the IMI
An average of the two or three test scores was made of the IMI scores after the balance circuit and of the scores after a session with Matti®. Figure 5 shows a bar chart of the mean IMI scores after the balance circuit sessions versus the sessions with Matti® for each child.
26
Figure 5: Average of the scores of the IMI
Three children scored higher on the IMI after the Matti® sessions, while eight children had a higher score on the IMI after the sessions with the conventional balance circuit. Due to missing data, it was not possible to apply statistics on the IMI.
Qualitative observations
Since the therapy was given in two different locations and the researchers had to use different materials, the balance circuits were different. Due to the fact that there was only one gaming mat available for the two locations, the mat was not always available when necessary. Furthermore, Matti® often did not work, resulting in missing data. Due to technical problems, the mat could not be used 12 times.
Another problem was the IMI to be time consuming. From the 30 minutes reserved for the intervention, it took at least 10 minutes to complete the IMI.
A third complication was the Likert scale where the numbers three to five were almost never used. Most of the participants chose number 'seven' when they agreed with the sentence and number 'one' when they did not.
27
Discussion
Most important results
The aim of this study was to evaluate the feasibility of the gaming mat 'Matti®' in paediatric rehabilitation, and the effect of exercising on the mat on balance and motivation with children with mild coordination and balance problems. The mat could be integrated into a traditional rehabilitation program. The results of the balance subtest of the M-ABC-2-NL and KTK-NL did not statistically improve after conventional therapy or intervention with Matti®. However, results following intervention with Matti® indicate a trend towards improvement, though not statistically different from baseline measures. The low number of participants could account for the lack of statistical significance. However, as this study was not a Randomised Control Trial (RCT), no conclusions regarding effectiveness can be made. The results of the IMI show no trend in the answers the children gave, with statistical analysis impossible as described before. There is no evidence to conclude whether there is a difference in motivation between therapy with or without the gaming mat. Higher scores can be found for eight children for the balance circuit, while only three children scored higher for the gaming mat. It should be noted that those differences in scores were considerably small, and could thus be neglected in broader research. To conclude, based on this pilot study, it is not possible to make a statement about the effectiveness of Matti® in improving balance, nor can it be shown that Matti® increases motivation.
A first reason why no clear statements can be made is the study design for this research. The participants underwent pre-post assessments without a control group. Originally the aim was to adopt a cross over design, however due to logistic constraints this was not possible. As such, the practice effect of repeated testing could not be monitored. The M-ABC-2-NL and the KTK-NL were assessed three times in a row for each participant, with only three weeks between measures. The study of Van Waelvelde et al. (2007) reported that repeated testing on the M-ABC-2-NL at intervals of three weeks results in a systematic measurement error (47). Therefore, the improvement shown in the results after the intervention with Matti® could be the result of a practice or learning effect of repeated testing. Particularly since most of the participants played only once or twice on the gaming mat. As the intervention with Matti® followed the balance circuit intervention, it could be possible that the children improved their balance scores by building on their already improved balance due to the balance circuit. It is also possible that balance improvements require more than three weeks to demonstrate significant change.
28 A second limitation of this study concerns the missing data. Not every child that participated attended the three test moments due to health problems, especially during the intervention with Matti®. Additionally, during the three weeks of the Matti® intervention, the gaming mat experienced repeated technical problems, preventing the gaming intervention from being carried out. At times there was no connection between the computer and the gaming mat, resulting in the mat not lighting up. Some participants could only play once during the three weeks intervention on Matti®, while others were able to play three times within three weeks. Lastly, the IMI was taken each week during the last 10 minutes of the session, after the intervention. In some circumstances a lack of time occurred to complete the questionnaire. Although almost all participants underwent the three weeks of the balance circuit therapy, not all of them were able to fill in the IMI. The IMI data collection was also affected by sessions in which the Matti® intervention did not work as expected. Comparing the average of three IMI's of the balance circuit to one IMI of Matti® could bias the results. Due to the missing data, the statistical power of this study is very low.
A third limitation relates to the standardisation of the assessment and intervention. Because of external factors, the proposed protocol was often disrupted. For example, unpredicted problems with time management arose due to the distractibility of the participants. It was feasible to comply with the time management during the Matti® intervention, as playtime was set to four minutes per game. However, this was more difficult to control during the balance circuit where participants were often slow to commence or move on from the exercises. Each week, the researchers designed a new balance circuit to maintain adequate levels of challenge for all participants. Nevertheless, some children performed better at the circuit than others, resulting in varied times required to complete each circuit. The researchers tried to adapt the circuit according to the level of the participant. However, this did not prove effective at normalising the speed of each participant of completion of the circuit. Some participants had to do the circuit in pairs due to time and equipment restraints, which may also have effected performance and outcomes. In pairs, the time to finish the circuit was often more than four minutes and may have contributed to the distraction exhibited by participants or may have affected motivation, thus resulting in the possible biases in the outcome measures. These problems did not occur during Matti® sessions. The games were all single-player and could be readily adjusted to the level of the child, ensuring appropriate challenge without impact on motivation or distraction. Additionally, the balance circuits differed between the two intervention locations. Furthermore, the testing moments were unable to be standardised due to absenteeism. To avoid more missing data, some test moments had to be rescheduled and took place directly following an intervention session. This could have affected the results as some participants may have decreased performance secondary to fatigue.
29 A distinction can be made between Matti® and other exergames. Firstly, little space is needed and the mat is easy to store. The mat is easy to use, especially for children with DCD. There are no other items required than the mat, a computer with internet accessibility and a screen to commence play. No boards could result in tripping hazards and no mandatory devices that they should hold in their hands. Nevertheless, there is sufficient space to practise balance on the mat according to its size. Additionally, researchers showed that a self-controlled exercise schedule, in which the participant can determine which game he or she wants to play, ensures a positive learning effect. This is based on the SDT (25). Due to access to a single mat between two locations, the mat did not always arrive at the beginning of each intervention session, resulting in decreased intervention time. This, together with the several technical break-downs of Matti®, could have affected the motivation of the children.
The Matti® system would benefit from improved ease of use. Games should commence with a brief demonstration outlining the goal of the game with specific instructions. An anti-slip coating lining the underside of the gaming mat would greatly improve safety, particularly of jumping games. The LED lights of the gaming mat should be brighter to improve visibility during daytime. The program of the mat should be more specific on what constitutes a “failed” exercise. Currently, when users jump three times when required to jump only twice the system determines that to be a correct attempt, while the researchers would argue this lack of control should constitute a “fail” score. Another suggestion would be to increase the sensitivity of Matti® to ensure it is able to differentiate between single and double leg exercises allowing the mat to differentiate jumping with one or two legs. This would also facilitate the inclusion of single leg static challenges while monitoring for the second leg touching down on the mat.
One of the research questions of this study was: ‘Does gamification, more importantly Matti®, increase motivation?’ To investigate this, the researchers used the IMI as assessment tool, based on the article of Choi et al. (2010) (48). The IMI is based on the CET (25), which states that intrinsic motivation derives from the need of the individual for autonomy, belonging and competence. The CET is a sub-theory of the SDT (27). The hypothesis that the intrinsic motivation of the child will enhance could not be analysed due to the low power of this study and the missing data, particularly following intervention with Matti®. Because the IMI was scheduled for the end of every session and required approximately 10 minutes to complete, a lack of time during sessions resulted in incomplete answering of questionnaires.
30 During data analysis and intervention reflection, researchers identified several issues with the IMI in determining motivation in this population. The primary concern was that the IMI was too long, resulting in children losing focus and concentration on questionnaire completion. This may have been confounded by taking the IMI at the end of each session when children were likely fatigued Another problem was that the language of the IMI proved to be too advanced for the younger participants, particularly for one who's native language was not Flemish. Most children did not understand the purpose of the seven numbers and how they could use them to nuance their responses to the Likert Scale. Most participants responded in a binary manner, choosing number 'seven' when they agreed with the sentence and number 'one' when they did not. Moreover, research by Choi et al. (2010) showed the IMI to be a reliable and valid instrument for assessing intrinsic motivation but is most suitable for people with at least a fourth-grade reading level (48). These issues may have contributed to the lack of conclusive findings for the IMI.
The SDT states that giving the children more autonomy influences their intrinsic motivation (26). As such, the researchers expected to see an increase in motivation while playing on the gaming mat. Each session the participants could choose three games to play on Matti®, with no limit to the number of times they selected the same games over the three weeks of intervention. Some children played the same game repeatedly, while others showed greater variation in the game selections. Studies have shown that variation in exercises is better for motivation than repeatedly doing the same exercises (49). Not only the gaming mat itself was determinative for the motivation, also letting the children choose their own game was a contributory factor. However, there was a lack of standardisation in the method of game selection with Matti®. Due to the variation in selection method, no conclusions can be made to see regarding the effect of increased autonomy on intrinsic motivation.
Overall, participants scored the IMI of the gaming mat lower than that of the balance circuits. This may be due to the technical and availability problems that occurred during the Matti® intervention sessions. Some participants stated feeling disappointed when the Matti® system did not work, which could have effected their motivation to play. It also should be noted that the researchers made an effort to make the balance circuits as attractive as possible for the children in an attempt to maximise enjoyment. The break from usual therapy of the participants and introduction of new therapists should not be discounted when analysing the expected enjoyment of the balance circuit interventions.
31
Future protocol
A blinded RCT, could be a cross-over design, is essential to prove the effectiveness of the gaming mat to enhance motor performance. The effect size of the study should exceed the value of the measurement bias. Power analysis is necessary to define the number of participants required to obtain an appropriate effect size, with consideration of high drop-out rates of participants. The intervention sessions should be adapted, with a longer duration for individual session and the intervention period. For example, conventional balance therapy could be compared to conventional balance therapy wherein the last 10 minutes consist of playing on the gaming mat, as the child desires. The effect on coordination and balance needs to be measured using validated outcome measures, e.g. the M-ABC-2-NL, the KTK-NL, the Bruininks-Oseretsky Test of Motor Proficiency (BOT), or another equally reliable outcome measure. The Goal Attainment Scales (GAS) could be used to evaluate the effect on patient-specific or parent-nominated activities, with motivation being measured through age-appropriate scales or questionnaires.
Future research should also ensure multiple testing sites always offer identical interventions, particularly concerning the balance circuits, ensuring the materials and difficulty adaptions are consistent regardless of testing centre. A prolonged study with more participants, a control group and a follow up test moment are recommended for future research.
32
Conclusion
Matti® seems to be a promising device to perform balance training with children. Effectiveness for improving balance or motivation in children has yet to be shown. No significant improvement was found in the balance scores of the M-ABC-2-NL and the KTK-NL, and no trend was found in the results of the IMI. Because of time constraints and missing data, the protocol required mid-testing alterations. A future protocol should account for difficulties experienced in this study to ensure more accurate and available data. In order to obtain sufficient statistical power and increase the level of evidence to consider the effect of Matti® in the rehabilitation of children with coordination and balance problems, a RCT comprising of a larger sample size and follow-up is recommended.
Since Matti® is not a task specific intervention, the improvement in Matti® scores does not necessarily transfer to daily life. A task-specific intervention, to expose a child repeatedly to a given balance task under specific constraints (e.g. the natural environment of the child), is currently one of the most common methods to improve the balance performance of children with DCD (50). This treatment strategy is based on the principles of motor learning and neuroplasticity (50). Research has shown that task-specific interventions can improve the motor performance of children with DCD in hopping, skipping and various balance activities (50). Children with balance impairments are recommended to train their balance in a task-oriented manner (e.g. training in the context and activity that proves difficult) (51). Giboin et al. (2015) reports that balance training improved performance only in the specific task that was trained with no transfer of balance skill to other tasks (51). Consequently, since Matti® has a process specific approach, it is not possible to say if this approach is effective. The outcomes of this study focussed solely on improved function and motivation and no task-specific assessments were conducted.
33
References
1. Macnab Jennifer J., Miller Linda T., Polatajko Helen. The search for subtypes of DCD: Is cluster analyses the answer? University of Western Ontario: Human Movement Science; 2001. p. 49 - 72.
2. Raghu L, Jea G, J. JM, P. HL, Matthew E, Alan E. The Association Between Developmental Coordination Disorder and Other Developmental Traits. University of Bristol, Bristol, United Kingdom: American Academy of Pediatrics; 2010. p. 1109 - 18.
3. Henderson SE, Henderson L. Toward an understanding of developmental coordination disorder: terminological and diagnostic issues.: Hindawi Publishing Corporation; 2003.
4. Joundi J., Penders A. The Design of an Interactive Surface for Supporting Rehabilitation of Children with Developmental Coordination Disorder. Ghent: Association for Computing Machinery; 2019. p. 335 - 44.
5. Deborah D. Developmental coordination disorder: Associated problems in attention, learning, and psychosocial adjustment. Department of Pediatrics, University of Calgary, Calgary, Alta. T2T 5C7, Canada: Human Movement Science; 2002. p. 905 - 18.
6. Geuze reint H. Postural Control in Children With Developmental Coordination Disorder. Developmental & Clinical Neuropsychology, University of Groningen, Grote Kruisstraat 2-1, The Netherlands: Hindawi Publishing Corporation; 2005.
7. Poulsen Anne A., Ziviani Jenny N., Johnson Helen, Cuskelly Monica. Loneliness and life satisfaction of boys with developmental coordination disorder: The impact of leisure participation and perceived freedom in leisure. Division of Occupational Therapy, School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Qld, Australia: Human Movement Science; 2008. p. 325 - 43.
8. Cairney J, Hay J, Faught B. Developmental coordination disorder and overweight and obesity in children aged 9-14 y. Department of Community Health Sciences, Brock University, St Catharines, ON, Canada: International Journey of Obesity; 2005. p. 369–72.
9. Piek Jan P., Baynam Grant. The relationship between fine and gross motor ability, self-perceptions and self-worth in children and adolescents. School of Psychology, Curtin University of Technology, G.P.O. Box U1987, Perth 6845, WA, Australia: Human Movement Science; 2006. p. 65 - 75.
10. Green D, Lingam R, Mattocks C. The risk of reduced physical activity in children with probable Developmental Coordination Disorder: A prospective longitudinal study. London: Research in Developmental Disabilities; 2011. p. 1332 - 42.
11. Pridmore T, Hons B, Cobb S, Hilton D, Green J, Eastgate R. Mixed reality environments in stroke rehabilitation: Interfaces across the real/virtual divide.: Virtual Reality & Assoc. Tech.; 2004.
12. Smits-Engelsman BCM, Jelsma LD, Ferguson GD, Geuze RH. Motor Learning: An Analysis of 100 Trials of a Ski Slalom Game in Children with and without Developmental Coordination Disorder. Plos One. 2015;10(10).
13. Smits-Engelsman BCM, Jelsma LD, Ferguson GD. The effect of exergames on functional strength, anaerobic fitness, balance and agility in children with and without motor coordination difficulties living in low-income communities. Hum Mov Sci. 2017;55:327-37.
34 14. Hammond J, Jones V, Hill EL, Green D, Male I. An investigation of the impact of regular use of the Wii Fit to improve motor and psychosocial outcomes in children with movement difficulties: a pilot study. Child Care Health Dev. 2014;40(2):165-75.
15. Jelsma D, Geuze RH, Mombarg R, Smits-Engelsman BCM. The impact of Wii Fit intervention on dynamic balance control in children with probable Developmental Coordination Disorder and balance problems. Human Movement Science. 2014;33:404-18.
16. Ashkenazi T, Weiss PL, Orian D, Laufer Y. Low-cost virtual reality intervention program for children with developmental coordination disorder: a pilot feasibility study. Pediatr Phys Ther. 2013;25(4):467-73.
17. Reis JRG, Neiva CM, Pessoa DM, Ciolac EG, Verardi CEL, Siqueira LOD, et al. Virtual reality therapy: motor coordination and balance analysis in children and teenagers with down syndrome. European Journal of Human Movement. 2017;38:53-67.
18. Jirikowic T, McCoy SW, Price R, Ciol MA, Hsu LY, Kartin D. Virtual Sensorimotor Training for Balance: Pilot Study Results for Children With Fetal Alcohol Spectrum Disorders. Pediatric Physical Therapy. 2016;28(4):460-8.
19. Biffi E, Beretta E, Diella E, Panzeri D, Maghini C, Turconi AC, et al. Gait rehabilitation with a high tech platform based on virtual reality conveys improvements in walking ability of children suffering from acquired brain injury. Conf Proc IEEE Eng Med Biol Soc. 2015;2015:7406-9. 20. Ju YJ, Du YC, Lin LY, Hou CR, Lin PY, Cherng RJ. The effect of laboratory-developed video games on balance performance in children with developmental coordination disorder. Biomedical Engineering-Applications Basis Communications. 2018;30(1).
21. Vangansbeke D, Veegaete T, Verdegem A. The Effect of 'Rehab Gaming' on Motivation for Balance Training in Children with Balance Disorders . Ghent University. 2017.
22. Flannery M. Self-Determination Theory: Intrinsic Motivation and Behavioral Change. Oncology Nursing Forum; 2017. p. 155-6.
23. Meyns P, Roman de Mettelinge T, Van Der Spank J, Coussens M, Van Waelvelde H. Motivation in pediatric motor rehabilitation: A systematic search of the literature using the self-determination theory as a conceptual framework. Developmental Neurorehabilitation; 2017. 24. Ryan Richard M., Deci Edward L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being. American Psychologist; 2000. p. 68-78.
25. Deci EL, Ryan RM. The general causality orientations scale: Self-determination in personality. University of Rochester: Journal Of Research In Porsonality; 1985. p. 109 - 14. 26. Deci EL, Eghrari H, Patrick BC, Leone Dean R. Facilitating internalization: The self‐ determination theory perspective. Journal of personality; 1994. p. 119-42.
27. Ryan RM. Control and information in the intrapersonal sphere: an extension of cognitive evaluation theory. Journal of Personality and Social Psychology, 1982; 1982. p. 450-61.
28. Adams N. Determination Theory. In: T.D. L, editor.: Development of Self-Determination Through the Life-Course. Springer, Dordrecht; 2017.
29. Przybylski AK, Rigby CS, Ryan RMK. A Motivational Model of Video Game Engagement. University of Rochester: American Psychological Association; 2010. p. 154 - 66.
35 30. George AM, Rohr LE, Byrne J. Impact of Nintendo Wii Games on Physical Literacy in Children: Motor Skills, Physical Fitness, Activity Behaviors, and Knowledge. Sports (Basel). 2016;4(1).
31. Sharan D, Ajeesh PS, Rameshkumar R, Mathankumar M, Paulina RJ, Manjula M. Virtual reality based therapy for post operative rehabilitation of children with cerebral palsy. Work. 2012;41 Suppl 1:3612-5.
32. Tarakci D, Ersoz Huseyinsinoglu B, Tarakci E, Razak Ozdincler A. Effects of Nintendo Wii-Fit((R)) video games on balance in children with mild cerebral palsy. Pediatr Int. 2016;58(10):1042-50.
33. Alvarez NG, Mortecinos AV, Rodriguez VZ, Fontanilla ML, Vasquez MM, Pavez-Adasme G, et al. Effect of an intervention based on virtual reality on motor development and postural control in children with Down Syndrome. Revista Chilena De Pediatria-Chile. 2018;89(6).
34. Salem Y, Gropack SJ, Coffin D, Godwin EM. Effectiveness of a low-cost virtual reality system for children with developmental delay: a preliminary randomised single-blind controlled trial. Physiotherapy. 2012;98(3):189-95.
35. Esposito M, Ruberto M, Gimigliano F, Marotta R, Gallai B, Parisi L, et al. Effectiveness and safety of Nintendo Wii Fit Plus (TM) training in children with migraine without aura: a preliminary study. Neuropsychiatric Disease and Treatment. 2013;9:1803-10.
36. Mombarg R, Jelsma D, Hartman E. Effect of Wii-intervention on balance of children with poor motor performance. Res Dev Disabil. 2013;34(9):2996-3003.
37. Hsieh HC. Effects of a Gaming Platform on Balance Training for Children With Cerebral Palsy. Pediatr Phys Ther. 2018;30(4):303-8.
38. Aprile I, Iacovelli C, Iuvone L, Imbimbo I, Cruciani A, Pecchioli C, et al. Use of a Virtual-Technological Sailing Program to Prepare Children With Disabilities for a Real Sailing Course: Effects on Balance and Quality of Life. J Child Neurol. 2016;31(8):1074-80.
39. Brown T, Lalor A. The Movement Assessment Battery for Children—Second Edition (MABC-2): A Review and Critique. Physical & Occupational Therapy In Pediatrics; 2009.
40. Stevens L, Tolleneer E. Identificatie van motorische stoornissen bij kleuters Universiteit Gent; 2009 - 2010.
41. Lenoir M. KTK-NL handleiding (Körperkoordinationstest für Kinder). 2014.
42. Plant RW, Ryan RM. Intrinsic motivation and the effects of consciousness, self-awareness, and ego-involvement: An investigation of internally controlling styles. Journal of Personality 53; 1985.
43. Edward M, Susan W, Terry DE. Self‐Efficacy, Perceptions of Success, and Intrinsic Motivation for Exercise. Journal of applied social psychology Volume 21 , Issue 2; 1991. p. 139-55.
44. Edward M, V. TV. The effects of subjective and objective competitive outcomes on intrinsic motivation. Sport and Exercise Psychology; 1989. p. 84-93.
45. Nikolaos T, Argiris T. Temporal stability of the intrinsic motivation inventory. Perceptual and Motor Skills, 2003, 97; 2003. p. 271-80.
46. Vera M, Mata L, Francisco P. Intrinsic motivation inventory: Psychometric properties in the context of first language and mathematics learning. Psicol. Reflex. Crit. vol.28 no.3 Porto Alegre July/Sept. 2015; 2015.
36 47. Van Waelvelde H, Peersma W. The reliability of the Movement Assessment Battery for Children for preschool children with mild to moderate motor impairment. Clinical Rehabilitation 2007.
48. Choi J, Mogami T, Medalia A. Intrinsic Motivation Inventory: An Adapted Measure for Schizophrenia Research. Schizophrenia Bulletin; 2010. p. 966–76.
49. Baz-Valle E, Schoenfeld BJ, Torres-Unda J, Santos-Concejero J, Balsalobre-Fernandez C. The effects of exercise variation in muscle thickness, maximal strenght and motivation in resistance trained men Plos One; 2019.
50. Fong SSM, Guo X, Liu KPY, Ki WY, Louie LHT, Chung RCK, et al. Task-Specific Balance Training Improves the Sensory Organisation of Balance Control in Children with Developmental Coordination Disorder: A Randomised Controlled Trial. scientific reports: Macmillan Publishers Limited; 2016.
51. Giboin L-S, Gruber M, Kramer A. Task-specificity of balance training. Human Movement Science; 2015.
37
Abstract (lekentaal)
Achtergrond: In de laatste decennia is het gebruik van interactieve computerspelletjes in de behandeling van kinderen toegenomen. Deze computerspelletjes worden verondersteld de motivatie te verhogen. De speelmat Matti® werd ontworpen door Creative Therapy met als doel om geïntegreerd te worden in de fysische revalidatie.
Doelstellingen: Het doel van de huidige studie was om de doeltreffendheid van Matti® te evalueren, in vergelijking met een gewoon evenwichtsparcours, om het evenwicht en de motivatie te verbeteren bij kinderen met milde coördinatie- en evenwichtsstoornissen.
Studie design: Een haalbaarheidsstudie gecombineerd met een piloot studie om de doeltreffendheid te evalueren van de mat, met als doel om evenwicht en motivatie te verbeteren. Methode: Twaalf kinderen (acht jongens en vier meisjes tussen zeven en 11 jaar) met evenwichtsproblemen namen deel aan deze studie. Elk kind startte drie weken therapie met behulp van een evenwichtsparcours gevolgd door opnieuw drie weken therapie, maar dan met de mat. Twee testen werden gebruikt om het evenwicht te bepalen bij het begin, na drie weken en na zes weken therapie. Om de mate van motivatie na te gaan, werd aan de kinderen gevraagd om na elke therapiesessie een vragenlijst in te vullen.
Resultaten: Er werd geen beduidende verbetering gevonden van de scores op de verschillende testen, over het verloop van de drie testmomenten.
Conclusie: Matti® lijkt een veelbelovend therapeutisch toestel om te werken aan het evenwicht bij kinderen. De doeltreffendheid moet nog bewezen worden, zowel voor het verbeteren van het evenwicht als voor het verbeteren van de motivatie.
38
46
Appendix
Appendix 1: Questionnaire IMI balance circuit
Interesse/ plezier
o Ik vond het evenwichtsparcours heel leuk o Ik had plezier tijdens het evenwichtsparcours o Ik vond het evenwichtsparcours saai
o Ik kon mijn aandacht helemaal niet bij het evenwichtsparcours houden o Ik zou het evenwichtsparcours beschrijven als heel interessant
o Ik vond het evenwichtsparcours redelijk plezierig
o Terwijl ik het evenwichtsparcours aan het spelen was, dacht ik na over hoe leuk ik het vond Ervaren competentie
o Ik denk dat ik redelijk goed ben in het evenwichtsparcours
o Ik denk dat ik het evenwichtsparcours heel goed deed, in vergelijking met andere kinderen o Nadat ik het evenwichtsparcours een tijdje gedaan had, voelde ik mij hier redelijk goed in o Ik ben tevreden over mijn prestatie op het evenwichtsparcours
o Ik deed het evenwichtsparcours redelijk goed o Ik kon het evenwichtsparcours niet heel erg goed Moeite/ belang
o Ik heb hier veel moeite voor gedaan/ mijn best gedaan
o Ik heb niet heel goed geprobeerd om het evenwichtsparcours goed te doen o Ik heb heel hard mijn best gedaan voor het evenwichtsparcours
o Het was belangrijk voor mij om het evenwichtsparcours goed te doen o Ik heb hier niet veel energie in gestoken
Druk/ spanning
o Ik voelde mij niet zenuwachtig terwijl ik dit aan het doen was
o Ik voelde mij heel gespannen terwijl ik het evenwichtsparcours aan het doen was o Ik was heel relaxed, rustig, ontspannen terwijl ik dit aan het doen was
o Ik was angstig terwijl ik het evenwichtsparcours aan het doen was o Terwijl ik dit aan het doen was, voelde ik mij onder druk gesteld Waarde/ nut
o Ik geloof dat het evenwichtsparcours een meerwaarde kan zijn voor mij o Ik denk dat het evenwichtsparcours nuttig zijn voor...
o Ik denk dat dit belangrijk is om te doen omdat...
o Ik zou dit graag nog eens doen omdat het een weerwaarde heeft voor mij o Ik denk dat het doen van het evenwichtsparcours mij kan helpen om... o Ik geloof dat het evenwichtsparcours nuttig/ voordelig kan zijn voor mij o Ik denk dat het evenwichtsparcours belangrijk is
47
Appendix 2: Questionnaire IMI Matti®
Interesse/ plezier
o Ik vond het spelen op de mat heel leuk o Ik had plezier tijdens het spel/ de spelletjes o Ik vond de spelletjes saai
o Ik kon mijn aandacht helemaal niet bij de spelletjes houden o Ik zou deze spelletjes beschrijven als heel interessant o Ik vond de spelletjes redelijk plezierig
o Terwijl ik de spelletjes aan het spelen was, dacht ik na over hoe leuk ik het vond Ervaren competentie
o Ik denk dat ik redelijk goed ben in deze spelletjes
o Ik denk dat ik deze spelletjes heel goed deed, in vergelijking met andere kinderen o Nadat ik deze spelletjes een tijdje gedaan had, voelde ik mij hier redelijk goed in o Ik ben tevreden over mijn prestatie op deze spelletjes
o Ik deed deze spelletjes redelijk goed
o Dit waren spelletjes die ik niet heel erg goed kon Moeite/ belang
o Ik heb hier veel moeite voor gedaan/ mijn best gedaan
o Ik heb niet heel goed geprobeerd om de spelletjes goed te spelen o Ik heb heel hard mijn best gedaan voor deze spelletjes
o Het was belangrijk voor mij om de spelletjes goed te doen o Ik heb hier niet veel energie in gestoken
Druk/ spanning
o Ik voelde mij niet zenuwachtig terwijl ik dit aan het doen was
o Ik voelde mij heel gespannen terwijl ik de spelletjes aan het spelen was o Ik was heel relaxed, rustig, ontspannen terwijl ik dit aan het doen was o Ik was angstig terwijl ik aan de spelletjes aan het spelen was
o Terwijl ik dit aan het doen was, voelde ik mij onder druk gesteld Waarde/ nut
o Ik geloof dat deze spelletjes een meerwaarde kunnen zijn voor mij o Ik denk dat deze spelletjes nuttig zijn voor...
o Ik denk dat dit belangrijk is om te doen omdat...
o Ik zou dit graag nog eens doen omdat het een weerwaarde heeft voor mij o Ik denk dat het spelen van deze spelletjes mij kan helpen om...
o Ik geloof dat het spelen van deze spelletjes nuttig/ voordelig kan zijn voor mij o Ik denk dat het spelen van deze spelletjes belangrijk is
48
Appendix 3: Thermometer
Appendix 4: Descriptives M-ABC-2-NL and KTK-NL for test moment 1, 2 and 3
M-ABC_1 M-ABC_2 M-ABC_3
Median 5,50 6,00 6,00 Minimum 1,00 1,00 1,00 Maximum 9,00 12,00 10,00 Percentile 25 2,50 2,00 2,00 Percentile 50 5,50 6,00 6,00 Percentile 75 8,75 9,00 9,00
49 KTK_BB_1 KTK_BB_2 KTK_BB_3 Median 77,00 76,00 81,00 Minimum 60,00 53,00 59,00 Maximum 124,00 112,00 109,00 Percentile 25 63,00 67,00 77,00 Percentile 50 77,00 76,00 81,00 Percentile 75 85,75 90,00 90,00 KTK_SJ_1 KTK_SJ_2 KTK_SJ_3 Median 65,00 78,00 77,00 Minimum 9,00 23,00 46,00 Maximum 94,00 94,00 111,00 Percentile 25 47,75 56,00 53,00 Percentile 50 65,00 78,00 77,00 Percentile 75 85,50 86,00 106,00